Background
• Temp >100.4°F/38°C
• Caused by response to bacteria, viruses, inflammation; ↑ metabolic rate, meds
• Distinct from hyperthermia (caused by exogenous factors)
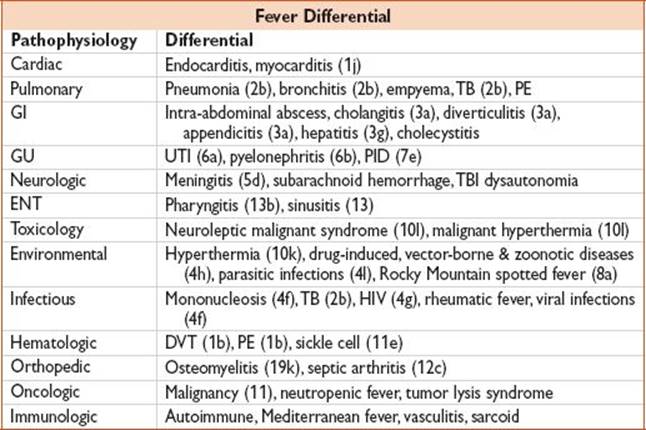
Approach
• Careful hx: COLDER, associated sxs (N/V, diarrhea, cough, abd pain, rash, AMS)
• Eval directed by pt hx & sx localization
• Assess VS for significant abnormalities that may indicate serious infection (↓ BP, ↑ HR)
• If immunosuppressed (HIV/AIDS, elderly, malnourished, chronic steroids, DM) or neutropenic, more intensive eval & testing: CBC, Chem, UA & cx, CXR; consider blood cx & admission
• Intermittent/relapsing fever, FUO, or occurring after foreign travel: Consider travel-related infectious etiologies, endocarditis
ENDOCARDITIS (Arch Intern Med 2009;169(5):463)
History
• RFs: IVDU, congenital or acquired valvular dz, prosthetic valves, structural heart dz, HD, indwelling venous catheters, cardiac surgery, bacteremia, chronic alcoholism, previous endocarditis
• Difficult to Dx 2/2 nonspecific sx (lethargy, weak, anorexia, low-grade temp), or negative w/u
Findings
• Fever (96%), new murmur (48%), CHF (32%), splenomegaly (11%), petechiae
• Classic physical exam findings
• Roth spots (2%): Exudative, edematous retinal lesions w/ central clearing
• Osler nodes (3%): Violaceous tender nodules on toes & fingers
• Janeway lesions (5%): Nontender, blanching, macular plaques on soles & palms
• Splinter hemorrhages (8%): Nonblanching, linear, reddish-brown under nails
• Septic emboli (mitral valve vegetations)
Diagnosis

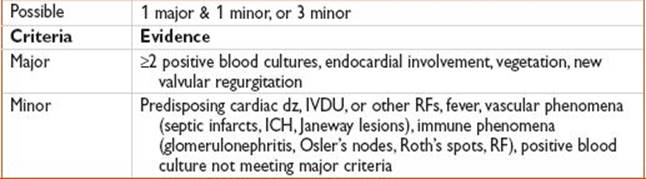
Evaluation
• EKG, CBC, Chem, coags; CXR, ↑ ESR/CRP (nonspecific), ≥2 blood cx
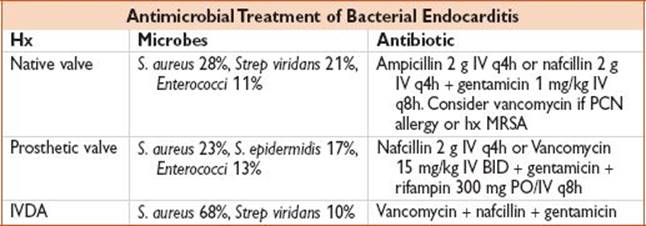
• Typically Staph or Strep species; also gram-negative bacilli, Candida (prosthetic)
• Echo for vegetations or valve ring abscesses; TEE more sens than TTE
Treatment
• Hemodynamic stabilization if valve rupture, can present w/ acute pulmonary edema cultures
• Immediate abx in suspected cases, preferably after blood cultures (see table)
Disposition
• Admit w/ continuous telemetry & IV abx, ICU if hemodynamic compromise
Pearls
• Infection of endothelium of heart (including but not limited to valves)
• Consider cardiac surgery consultation for refractory CHF, fungal endocarditis, recurrent septic emboli, conduction disturbance, persistent sepsis, aneurysm rupture of sinus of Valsalva, kissing infection of anterior mitral leaflet w/ aortic valve endocarditis
• Mortality w/ native valve dz: ∼25%; prosthetic valve higher
• Worse prognosis if involves aortic valve, DM, S. aureus (30–40%)
• Left-sided endocarditis (mitral 41%, aortic valve 31%) most common
• IVDU: Tricuspid valve endocarditis; rheumatic valve dz: Mitral, then aortic valve