INFECTIOUS DISEASES
FEVER SYNDROMES
Temperature >101°F or >38.3°C
Diagnostic approach
• Thorough history including ROS, PMH/PSH, immunizations, including from childhood
• Fever curve (consider holding antipyretics); less likely to mount fever if: chronic renal or liver dis., extremes of age, protein calorie malnutrition, immunosupp., steroid use
• Exposures: travel, occupation or hobbies, animals and insects, sexual contacts, TB; consider age, geography, season and incubation time in relation to exposures
• Physical exam: complete exam w/ focus on mucuous membranes & conjunctiva; cardiac murmurs; liver and spleen size; skin, genitals, lymph nodes, & joints; complete neuro exam incl cranial nerves and meningeal signs
• If rash: location, duration, progression/∆ in appearance, was prodrome present
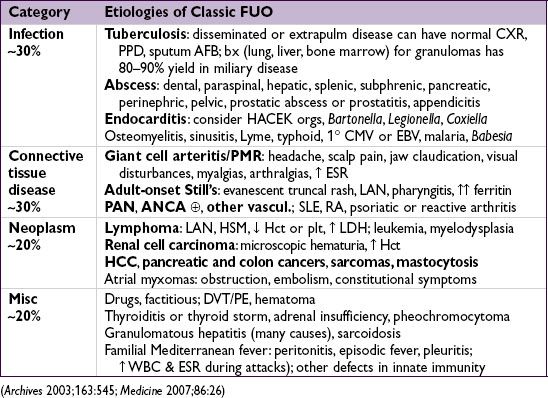
FEVER OF UNKNOWN ORIGIN (FUO)
Definition & etiologies
• Fever (as per above def) on >1 occasion during ≥3 wk & no dx despite 1 wk of evaluation
• More likely to be subtle manifestation of common disease than an uncommon disease
• In Pts with HIV: >75% causes are infectious, but rarely due to HIV itself
• Frequent reassessment needed to identify focal signs and progression of disease
Workup
• Focus by H&P, incl: CBC w/ diff, lytes, BUN, Cr, LFTs, ESR, CRP, ANA, RF, cryoglobulin, LDH, CK, SPEP, 3 sets BCx (off abx), U/A, UCx, PPD or IGRA, HIV Ab ± PCR, heterophile Ab (EBV serologies if ![]() ), CMV antigen, Hep serologies if LFTs abnl
), CMV antigen, Hep serologies if LFTs abnl
• Stop unnecessary meds (only 20% with a med cause have eos or rash), reassess 1–3 wk
• Imaging: CXR, chest & abd CT, consider tagged WBC, gallium scan, PET, TTE, LENI
• Duke’s criteria for endocarditis (qv) have good Se & Sp in Pts with FUO
• Consider temporal artery bx if ↑ ESR and age >60, particularly if other s/s
• ? Bone marrow aspirate & bx (esp. if signs of marrow infiltration) or liver bx (esp. if ↑ Af): even w/o localizing s/s, yield may be up to 24% (path and culture) (Archives 2009;169:2018)
• Pursue abnormalities raised by above w/u (eg, bx, MRI, etc., for dx, not screening)
Treatment
• Empiric abx not indicated (unless Pt neutropenic)
• Empiric glucocorticoids not indicated unless strong suspicion for specific rheumatologic dx
• Up to 30% of cases remain undiagnosed, most spontaneously defervesce (wks to mos)
FEVER AND RASH
Approach to diagnostic workup
• Meningococcemia, IE, RMSF, sepsis, toxic shock require immediate dx & Rx
• Workup: CBC w/ diff, lytes, BUN/Cr, LFTs, LDH, CK, U/A, HIV Ab ± PCR, BCx (off abx)
• To narrow Ddx: characterize time course of rash, progression & morphology (ie, vesicular, maculopapular, pustular, purpuric, ulcerative)
• Erythema multiforme: symmetric “target” lesions often of palms, soles, & mucous memb
Infxn etiol: HSV 1/2, Mycoplasma, syphilis, tick borne diseases, etc.
Non-infxn etiol: meds (eg, NSAIDs, sulfa), malignancy, autoimmune & rheum disease
• Erythema nodosum: tender erythematous or violaceous nodules usually symmetric on LE
Infxn etiol: Strep, TB, EBV, Bartonella, HBV, psittacosis, fungal, L. venereum, etc.
Non-infxn etiol: sarcoidosis, IBD, Behçet’s, other rheum, pregnancy/OCP use
• Pursue specific dx based on exposure hx & exam, including serologies, viral swab PCR, antigen tests and possibly skin biopsy ± exam of vesicular or bullae fluid if present
• Etiologies more broad in immunosupp. Pts, and dx approach usually more extensive; higher risk of critical illness due to disseminated or rapidly progressive infxns

Treatment
• Empiric abx are not indicated (unless Pt neutropenic or critically ill)
FEVER IN A RETURNED TRAVELER
Definition & etiologies
• Febrile illness after recent travel outside of U.S./Canada; Ddx is extensive:

• Pts visiting friends and relatives abroad are most likely to contract illness during travel
• Emerging pathogens: Influenza occurs year round in the tropics. Chikungunya and dengue w/ ↑ areas of transmission, hemorrhagic fevers primarily in Central Africa.
• Consider domestic infxns, STIs, & non-infxn causes. Enteric parasites rarely cause fever.
Select clinical manifestations
• Malaria: nonspecific symptoms including diarrhea, myalgias, cough, altered mental status
• Dengue: nonspecific symptoms including headache, severe myalgias, rash/petechiae
• Typhoid: constipation, abdominal pain, possible rash, relative bradycardia
• Rickettsial disease: headache, myalgias, lymphadenopathy, possible rash/eschar
Workup
• Routine testing: CBC w/ diff, lytes, LFTs, BCx, UA, rapid malaria test
• Fever in a traveler from a malaria zone is malaria until proven otherwise; consider hospitalization and empiric Rx. One ![]() smear does not r/o malaria.
smear does not r/o malaria.
• Other tests based on s/s, labs, exposure, incubation period, geography and seasonality. O&P exam, CXR, blood smears for filaria/Babesiosis/Borrelia, serologies, STI & HIV, PPD or IGRA, bone marrow aspirate, bx of lymph nodes or skin lesions, CSF studies.