Definition
• A form of acute lung injury seen in neonates as a result of immaturity and surfactant deficiency; the pathologic correlate of neonatal respiratory distress syndrome
Clinical features
Epidemiology
• Affects approximately 1% of infants born worldwide
• Incidence inversely proportional to gestational age and birth weight: 60% to 80% in infants less than 28 weeks of gestational age, 15% to 30% in those between 32 to 36 weeks, 5% in infants more than 37 weeks
• Rarely, it occurs in mature infants when it is due to dilution of surfactant (inadequate resorption of lung liquid at birth)
• Risk factors include prematurity, white race, male sex, maternal diabetes, birth by cesarean section, multiple gestation, precipitous delivery, asphyxia, cold stress, and a maternal history of prior affected infants
Presentation
• Clinical signs of respiratory distress
• Clinical presentation manifests almost always before 8 hours of age (if symptoms develop after 8 hours of normal breathing, hyaline membrane disease is excluded)
• Typical radiographic finding includes diffuse, bilateral, “granular” opacities with superimposed air bronchograms
Prognosis and treatment
• Best prevention is avoidance of premature labor and delivery
• Antenatal betamethasone therapy is helpful in preventing hyaline membrane disease
• Key treatment measures include exogenous surfactant therapy, oxygen therapy, and mechanical ventilation
• Milder cases usually peak at 2 to 3 days of age; gradual improvement follows
• Infants with severe or untreated disease may develop bronchopulmonary dysplasia or may die of the disease
• Advances in prevention and treatment have decreased mortality and the incidence of subsequent bronchopulmonary dysplasia and markedly improved chances of survival
Pathology
Gross
• Lungs are firm, solid, red, congested, and sink in water
• Relatively airless cut surface with marked atelectasis and a liver-like appearance
Histology
• Alveolar sacs lined by hyaline membranes, which consist of epithelial debris, fibrin, amniotic fluid, and transudate fluid proteins
• Although hyaline membranes start to form within 30 to 60 minutes of high oxygen and respirator therapy, it takes approximately 4 hours of breathing room air for hyaline membranes to be well developed; therefore, hyaline membranes may be inconspicuous in infants who die at less than 4 hours of age
• Hyaline membranes are not specific and may be present in other conditions (see differential diagnosis)
• Immaturity of lung tissue usually apparent (airspaces without hyaline membranes lined by cuboidal epithelium)
• Surrounding lung tissue with congestion, hemorrhage, epithelial desquamation, and lymphatic dilatation
• Atelectasis of distal airspaces and overdistension of proximal airspaces
Immunopathology/special stains
• Not contributory
Main differential diagnoses
• Other conditions with the presence of hyaline membranes, such as meconium aspiration and viral or bacterial infections
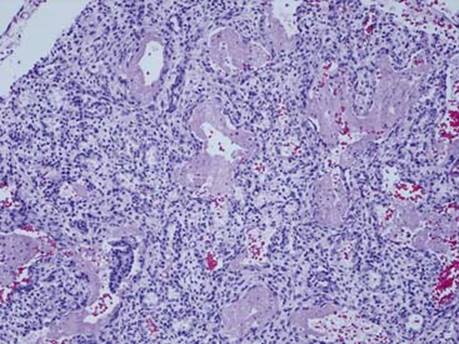
Fig 1 Hyaline membrane disease. A section of the lung from a newborn of 24 weeks’ gestational age. Open alveolar sacs are lined by homogenous eosinophilic hyaline membranes. The surrounding alveolar sacs are atelectatic and show evidence of immaturity (lined by cuboidal epithelium).
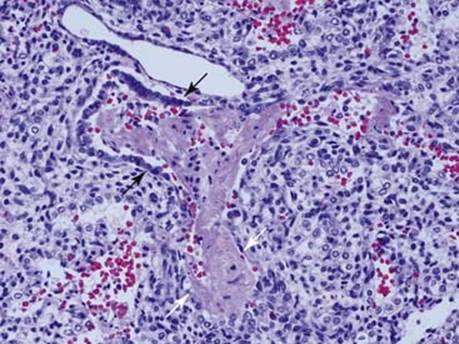
Fig 2 Hyaline membrane disease. High-power view of hyaline membranes involving terminal bronchiole (black arrows) and extending into alveolar sac (white arrows). Note the cuboidal epithelium is partially preserved at the bottom of the alveolar sac.
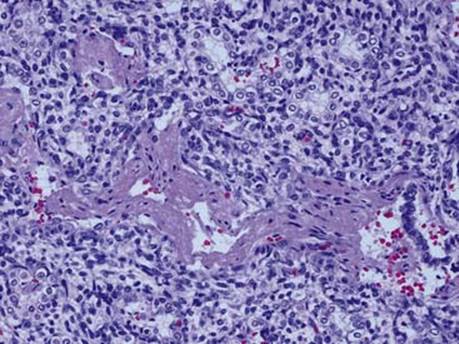
Fig 3 Hyaline membrane disease. Collapsed airspaces lined by cuboidal epithelium are evident adjacent to (above and below) bronchiole and airspaces involved by hyaline membranes.