Definition
• Rare benign neoplasm of neural crest origin arising from the sympathetic ganglia; composed of mature ganglion cells in a dense Schwannian stroma
Pathogenesis
• Tumor may arise de novo or as a result of differentiation from a neuroblastoma
• Some cases arise from treated neuroblastomas
• Differential signaling in hedgehog pathway, as seen through higher levels of Gli1 expression, leads to greater differentiation of tumors, resulting in a ganglioneuroma phenotype
• Requisites for differentiation of a neuroblastoma include an intact chromosome 1 short arm, nonamplified MYCN, and DNA near-triploidy (see Mediastinal Neuroblastoma chapter)
• Absence of these requisites may result in proliferation of neuroblastic cells rather than differentiation
Clinical features
Epidemiology
• Typically affects older children, adolescents, and young adults; mean age at diagnosis, about 6 years
• Female to male ratio about 1.5:1
• Most commonly occurs in the posterior mediastinum; may occur in retroperitoneum or adrenal medulla
Presentation
• About half of patients are asymptomatic and are given a diagnosis after radiological chest imaging for other reasons
• Some patients may have increased serum levels of vanillylmandelic acid and homovanillic acid along with vasoactive symptoms
• Tumor may grow to impinge on other thoracic structures or grow into the spinal canal in a “dumbbell” fashion, producing pain and/or paresthesias
• Radiological imaging shows a well-circumscribed mass spanning three to five vertebral processes; it may impinge on the spine, causing pressure erosion with sclerotic borders
• Punctate calcification may also be seen radiologically
Prognosis and treatment
• Ganglioneuromas are largely benign tumors, although rare cases of metastasis have been reported, of which some were believed to be neuroblastomas that have metastasized and subsequently matured
• Treatment is complete excision; recurrence is rare
Pathology
Gross
• Tumors are often large, oblong, and encapsulated. The cut surface is bulging and yellow-tan with areas of trabeculation
Histology
• There are ganglion cells (large cells with eccentric nuclei, vesicular chromatin, a prominent nucleolus, and amphophilic cytoplasm) arranged singly or in clusters
• The stroma is characteristically Schwannian with a fibrous appearance and no neuropil
• Satellite cells may be found surrounding the ganglion cells
• No neuroblastic cells are seen in the mature subtype; however, the maturing form has a mixture of neuroblasts and ganglion cells
Immunopathology/special stains
• Not contributory
Main differential diagnoses
• Neuroblastoma: will not have many ganglion cells; caution must be taken when the tumor invades normal ganglion structures
• Ganglioneuroblastoma: the stroma constitutes >50% of the tumor in contrast to ganglioneuromas and demonstrates foci of neuroblastic cells

Fig 1 Mediastinal ganglioneuroma. Grossly, the lesion has a homogenous, white-tan cut surface. No areas of hemorrhage or necrosis are present.

Fig 2 Mediastinal ganglioneuroma. This scan of the whole slide shows uniform pink tumor without areas of high cellularity.

Fig 3 Mediastinal ganglioneuroma. Low power shows an encapsulated tumor. A cluster of ganglion cells is surrounded by a moderately dense fibrous stroma.

Fig 4 Mediastinal ganglioneuroma. At medium power, the ganglion cells appear mature and are set within a Schwannian-rich stroma.

Fig 5 Mediastinal ganglioneuroma. At high power, the neoplastic ganglion cells have abundant pink to amphophilic cytoplasm, indicative of Nissl substance, and eccentric, enlarged nuclei, each with a prominent single nucleolus. Maturity of the ganglion cells is seen here by the presence of satellite cells (arrows).
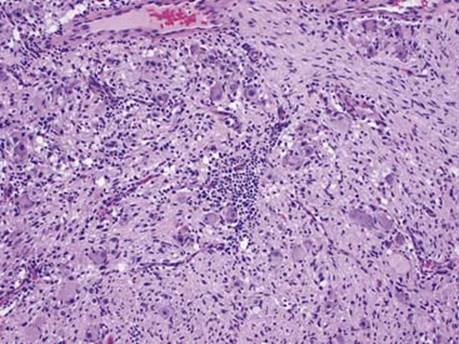
Fig 6 Mediastinal ganglioneuroma. This tumor from the posterior mediastinum of a 46-year-old shows intermixed lymphocytes, which should not be mistaken for neuroblasts.

Fig 7 Mediastinal ganglioneuroma. Mature ganglion cells and Schwannian stroma with many lymphocytes and some plasma cells in the same case as Fig 6.