Definition
• Segment of abnormal lung with no connection to the tracheobronchial tree with its own anomalous systemic arterial blood supply, most commonly occurring on the left side
• Part of the spectrum of bronchopulmonary foregut malformation complex
• Two types: intralobar sequestration (ILS), extralobar sequestration (ELS)
Clinical features
Epidemiology
• ILS is seen in older children and adults; might be acquired; male:female (M:F) ratio is 1:1
• ELS is a true congenital malformation and is seen in younger children (<1 year), M:F is 3-4:1
Presentation
• ILS patients commonly have recurrent pulmonary infections, chest pain, and coughs. Roughly 30% of the patients are asymptomatic, and the sequestration is an incidental finding on chest imaging
• ELS usually is seen in association with other congenital anomalies such as congenital diaphragmatic hernia, vertebral anomalies, congenital heart disease, pulmonary hypoplasia, colonic duplication shortly after birth
Prognosis and treatment
• Treatment is supportive. Surgery is the only definitive treatment
Pathology
Gross
• ILS: the lesion is within a lung lobe but is isolated from the tracheobronchial tree and has its own arterial blood supply
• ELS: the lesion is a discrete mass of pulmonary parenchyma, outside the lung with its own pleura and systemic arterial supply
Histology
• Intralobar (ILS)
• Sharply demarcated from the adjacent normal lung parenchyma, with no pleura
• Replacement of lung parenchyma by chronic inflammation with mucus accumulation and microcyst formation
• Remnants of bronchi and bronchioles within a dense fibrotic stroma with numerous lymphocytes
• A vascular pedicle and thickening of the overlying pleura may be present
• Extralobar (ELS)
• Circumscribed mass, covered with visceral pleura, independent of the normal lung
• Irregular, enlarged (2×-5×) bronchi, bronchioles, and alveoli
• Bronchial structures with normal to irregular lumens lined with pseudostratified columnar epithelium may be present
• No significant inflammation or fibrosis
• Dilated subpleural lymphatics may be present
• Areas of congenital pulmonary airway malformation (CPAM) type 2 can be identified in half of the cases
Immunopathology/special stains
• Not contributory
Main differential diagnoses
• Other cystic lung lesions devoid of an independent systemic blood supply
• CPAM
• Bronchogenic cyst
• Congenital lobar emphysema
• Primary lung abscess
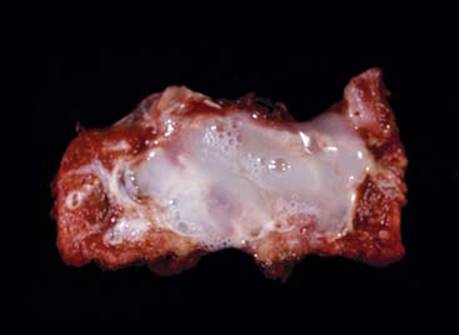
Fig 1 Pulmonary sequestration. Intralobar sequestration; gross image of cut surface shows large cystic space filled with mucus.
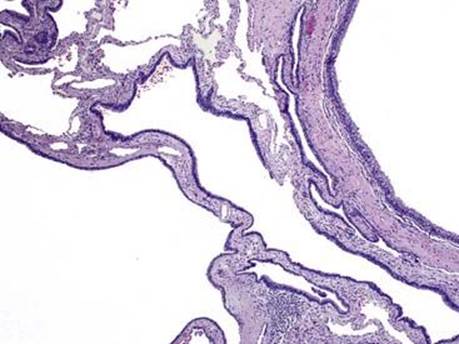
Fig 2 Pulmonary sequestration. A 5-month-old with ILS with CPAM type 2 (microcyst formation, lined by bronchiolar epithelium).
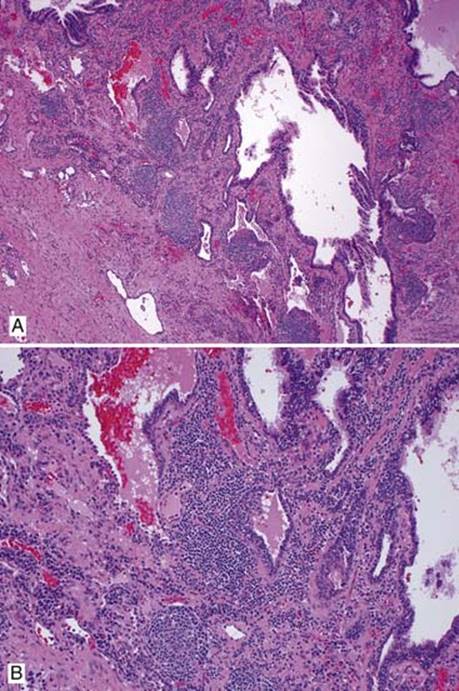
Fig 3 Pulmonary sequestration. ILS in an 11-year-old, associated with chronic inflammation and fibrosis; low (A) and high (B) powers.
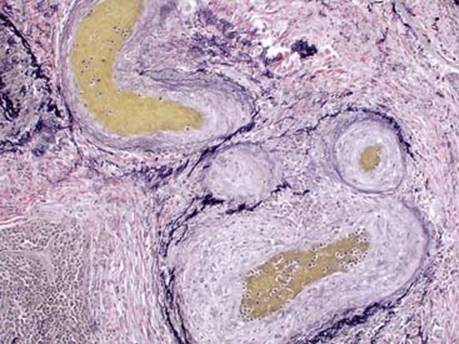
Fig 4 Pulmonary sequestration. ILS in a 34-year-old; elastic stain shows marked secondary pulmonary arterial hypertension with intimal fibrosis.
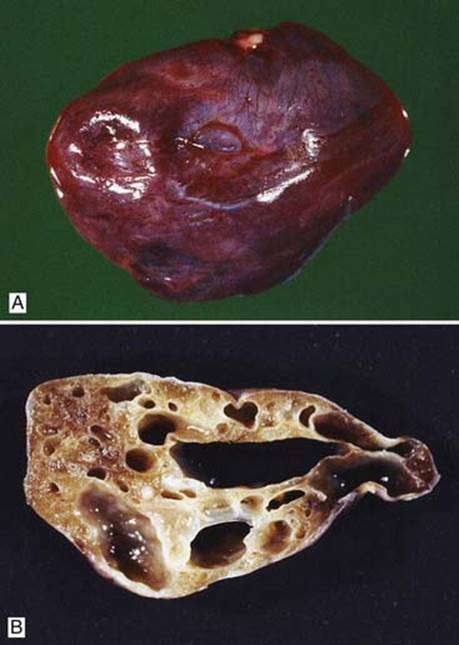
Fig 5 Pulmonary sequestration. Gross image of ELS: resected specimen (A) and cut surface (B).
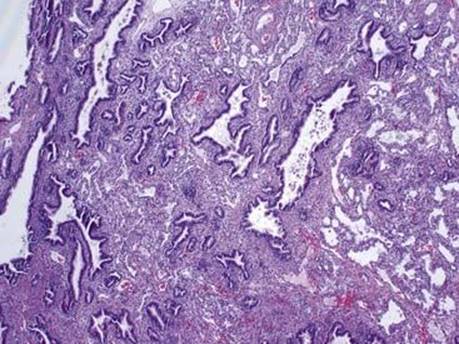
Fig 6 Pulmonary sequestration. ELS, bronchial structures with normal to irregular lumens lined with pseudostratified columnar epithelium (CPAM type 2).