Justin M. Watts and Dan Douer
Lymphoblastic Neoplasms can present as leukemia or lymphoma
→ ALL: ≥20% BM blasts
→ Acute LBL: <20% BM blasts + mass lesion
• ALL & LBL are essentially the same disease & are treated similarly
• ALL/LBL can be further classified by lineage → precursor B or T cell ALL
• 6070 cases annually in US (2% of all lymphoid neoplasms); more common in children; median age in adults is 39 y; higher incidence in Hispanics
Clinical Presentation
• Aggressive malignancy that presents similarly to AML w/pancytopenia & circulating blasts; common s/s → fatigue, pallor, infxn, bleeding
• LAN & HSM are more common in ALL > AML
• Anterior mediastinal mass → suggests T-ALL
• Pts may have bony pain
• CNS involvement (15%): Usu cranial neuropathies/leukemic meningitis, but can be mass lesion; more common in T-ALL
• TLS more common in ALL > AML; can be spontaneous from rapid cell turnover & ↑ w/initiation of CT; 1st signs ↓ Ca, ↑ LDH, followed by ↑ K, ↑ Phos, ↑ UA → complications include renal failure & cardiac arrhythmias (also see AML section)
• DIC (check coags & fibrinogen) & leukostasis can occur in ALL, esp. if WBC >100000/μL
Diagnosis & Disease Biology
• BM morphology: Hypercellular marrow usu replaced w/lymphoblasts (unless LBL) → absence of granules/Auer rods; also obtain flow cytometry & cytogenetics
• Histochemical stains/flow: (+) TdT in 95% of ALL
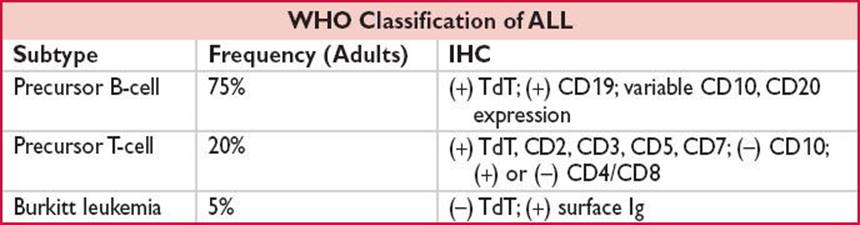
• B-ALL can be further subdivided into:
→ Early pre-B ALL (pro-B ALL): (+) CD19, (+) CD79a, (+) cCD22, (–) CD10
→ Common pre-B ALL: (+) CD10
→ Late pre-B ALL: (+) CD20, (+) cytoplasmic mu heavy chain
• T-ALL can be further subdivided into:
→ Early/pro-T cell ALL: (+) CD2, (+) CD7, (+) CD38, (+) cCD3
→ Common T-cell ALL: (+) CD1a, (+) CD3, (+) CD4/CD8
→ Late T-cell ALL: (+) CD4 or (+) CD8
• NOTCH gene Mt important role in T-ALL
• LP in pts w/suspicion of CNS disease (can be sanctuary site); image first in pts w/neurologic s/s; IT chemotherapy usu given w/diagnostic LP (as CNS involvement common & to prevent seeding from circulating blasts/traumatic tap)
• Testicular exam as well (also potential sanctuary site)
• CT chest to r/o mediastinal mass (if T-cell lineage)
• Transthoracic echocardiography before beginning Rx w/anthracyclines
Prognosis is better in children
• Most pts will achieve CR → >90% of adults
• Many pts w/ALL can be cured w/chemotherapy alone
• The role of allogeneic HCT as postremission Rx is not well defined
• The cure rate in adult ALL remains ∼35–40% but varies depending on prognostic features → ranging from 10–30% w/unfavorable-risk features to 50–70% w/favorable-risk features
• Favorable prognostic features: Children/adolescents/younger adults; WBC <30000/μL for pre-B cell ALL; <100000/μL for T-ALL; rapid achievement of CR; hyperdiploidy (>50 chromosomes); t(12;21) → more common in childhood ALL
• Poor prognostic features: Infants (<1 y) & older adults; t(9;22)/Ph chromosome (although w/advent of TKIs this may be changing); t(4;11) or any translocation involving MLL/11q34 gene rearrangements (NEJM 2004;351:533)
Treatment of Ph-ALL (NEJM 2006;354:166)
• Induction: Multiple published combination CT regimens, no clear standard of care → ∴NCCN recommends considering clinical trial as first-line option
• Repetitive courses of postremission CT (consolidation/intensification) over 6–8 mos, followed by maintenance CT (1–2 y)
• A commonly used regimen in adults is Hyper CVAD, w/c alternates between parts A & B
→ Part A: Hyperfractionated cyclophosphamide, doxorubicin, vincristine, dexamethasone
→ Part B: HD-MTX & high-dose cytarabine
• Other adult regimens have adopted the Berlin–Frankfurt–Munster (BFM) model, w/c has been shown to be safe in young & middle-aged adults (originally developed in children) & may improve survival
• BFM model-based regimens include anthracyclines, cyclophosphamide, cytarabine, vincristine, steroids, asparaginase; 2-phase induction & planned “re-induction”
• Pediatric strategies now utilized in adult ALL → greater use of nonmyelosuppressive agents such as steroids, vincristine, & asparaginase (prolonged asparagine depletion), ↑ /more frequent CNS ppx w/IT CT, systemic HD-MTX (penetrates CNS), long-term maintenance Rx

• CNS irradiation if documented CNS disease
• No clearly defined role for allogeneic HCT in first CR, but should be considered in pts w/poor-risk features, eg, t(4;11)
• If relapse, salvage CT followed by allogeneic HCT if appropriate
• Novel agents, such as blinatumomab in B-ALL & NOTCH inhibitors in T-ALL, being studied in relapsed/refractory disease
• CAR-modified T cells also being studied in ALL
• Supportive care: Includes mgmt of TLS (hydration, allopurinol, rasburicase for ↑↑ UA) & DIC (FFP, cryo, PLT transfusions), broad-spectrum abx for FN, antibiotic ppx for prolonged neutropenia
Treatment of Ph+ ALL (25% of adult ALL)
• More common in the elderly & carries a poor-risk
• Philadelphia chromosome/t(9;22) usu p190 subtype (p210 = CML)
• Addition of TKI such as imatinib(Blood 2004;103:4396) or dasatinib to CT have improved outcomes → start TKI w/induction Rx & continue indefinitely (may have to hold transiently if delayed count recovery after induction CT)
• W/advent of TKI, OS in adult Ph+ ALL has improved to ≥50%
• Role of allogeneic HCT & duration of TKI Rx (w/or w/o transplant) still being investigated in Ph+ ALL
• In older or unfit pts, steroids + TKIs (± vincristine) are well-tolerated & can be used w/high remission rates