James J. Harding and Eileen M. O’Reilly
Definition
Cholangiocarcinomas (CC), tumors of the bile duct (BD) epithelium, differentiated by anatomic site of origin.
Intrahepatic (10%)
Hilar (40%), confluence of R/L hepatic duct (Klatskin tumor)
Distal (50%), involve CBD/Ampulla of Vater
Extrahepatic CC = hilar + distal CC
Gallbladder carcinoma (GBC) is histologically = CC but ≠ epidemiology, staging system, & surgical tx
Anatomic site of origin → fundus (60%), body (30%), neck (10%)
Epidemiology
Incidence: ∼10000 new cases/y & ∼3200 D/y in US of CC & GBC; GBC is more common
Most cases are sporadic (NEJM 1999;341:1368)
↑ Risk w/adv age, ↑ risk w/chronic inflammation
CC specific RFs → PSC, choledochal cysts, Asian liver flukes (O. viverrini & C. sinensis), chronic calculi of BD, HCV, HBV, & male sex
GBC-specific RFs → chronic cholelithiasis, GB calcification (ie, porcelain GB), & female sex
Pathophysiology
Most common histological subtype = adenoca (90% CC, 80% GBC), less common: Small cell CA, SCC, sarcomas
Underlying molecular biology & pathogenesis of GBC & CC is poorly understood, Mts are found in p53, KRAS, BRAF, c-MET, PIK3CA, HER2/neu, & EGFR (JCO 2010;28:3531)
Clinical Manifestations
Sx depend on location of lesion; include painless jaundice, pruritus, abdominal pain, biliary colic (especially in GBC), cholangitis, clay-colored stool, cola-colored urine, fevers, anorexia, & wt loss
Exam: Hepatomegaly, palpable GB due to obstruction of cystic duct (Courvoisier sign), jaundice, ascites
Labs & initial studies: ↑ T-bili, ↑ AST/ALT, ↑ γ-GT, US-ABD (±) stones
Diagnostic Evaluations
MRI/MRCP or CT-A/P (multiphase delayed contrast)
Determines anatomy, location & degree of obstruction
Used to plan for bx, surgery and/or stenting
ERCP or PTC: Commonly employed but not required in all cases
ERCP to stent, relieve obstruction, & to bx (cytology, brushings)
If ERCP is non-diagnostic consider EUS or CT-guided for FNA/core
In cases w/suspicious lesion w/o biliary obstruction & distant disease → surgery w/o bx
CA19-9 & CEA, CT-Chest, questionable role for PET
Staging and Prognosis
Four unique AJCC TMN staging systems for CC (intrahepatic, hilar, distal) & GBC
Key differences for staging systems: Intrahepatic T stage based on # of lesions & similar to HCC staging while hilar, distal & GBC T staging reflects degree of invasion through BD epithelium
AJCC staging may not adequately predict surgical resectability (specifically for hilar, consider Bismuth or Blumgart classification)
OS in met setting is poor:
GBC Stage IV → 5-y OS <1%, median OS ∼6 mos
Intrahepatic CC Stage IV → 3 y OS ∼10%, median OS ∼13 mos
Surgical Treatment
Early surgical consultation is critical for CC & GBC
R0 resection improves OS; surgery is the only curative Rx
Avoid needless biliary stenting in resectable pt, no advantage to preoperative biliary decompression (Ann Surg 2002;236:17)
Staging laparoscopy may be required in select cases
Intrahepatic CC Resection
Requires hepatic lobectomy
Contraindication to surgery: Multifocal tumor, extrahepatic extension, & N1 disease
5-y OS s/p resection ∼15–40%
Extrahepatic CC resection
Hilar→ en bloc resection hepatic lobe + involved extrahepatic BD + periportal LND; if L main hepatic duct → caudate lobectomy
Distal → Pancreaticoduodenectomy + extrahepatic BD to confluence (high surgical morbidity & mortality)
5-y OS s/p resection ∼10–40%
GBC
Often laparoscopic surgery for suspected gallstones, incidental CA
Only a T1a lesion can be treated w/simple cholecystectomy (CCY)
Extended (radical) CCY → en bloc resection of GB, wedge resection of GB bed (Seg IVb & V), regional LND
If jaundiced at presentation, curative surgery unlikely
5-y OS depends on T stage, approaches 100% T1, 0–40% T3/T4
Systemic and Local Regional Treatment
Adjuvant Rx: Limited clinical data due to the rarity of the disease; mostly small phase II clinical trials or retrospective series; participation in clinical trials recommended (JCO 2012;30:1934)
Observation is recommend for T1 GBC (long-term OS ∼100%)
Observation can be considered for R0 & N0 intra/extrahepatic CC
In all other cases, adjuvant Rx is recommended due to the high risk of local regional & met recurrence
For R1/R2 intrahepatic CC resections, consider re-resection or ablation
Typical adjuvant regimens: Fluoropyrimidine chemoRT, fluoropyrimidine- or GEM-based chemotherapy
Surveillance & Tx of Recurrence: Serial exam, CT-CAP, CA19–9, CEA q6mos for 2 y than annually, if local recurrence → chemoRT (if none prior), ablation, re-resection or chemo alone; if met see below
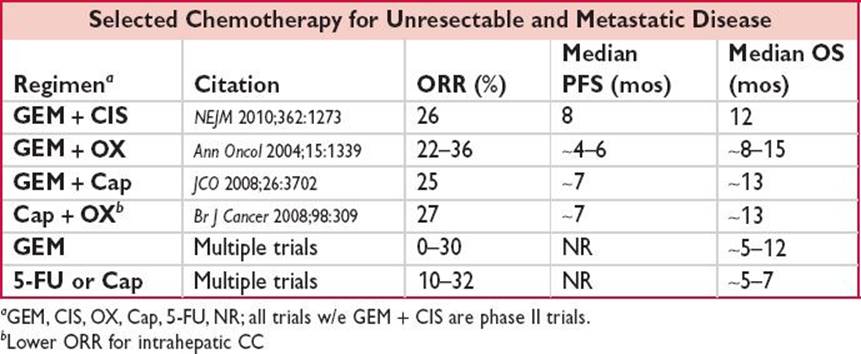
Tx for Unresectable & Met Disease
Systemic chemotherapy
ABC-02: Randomized Phase III of GEM + CIS vs. GEM in 410 pts w/adv GBC, CC, ampullary CA; GEM + CIS superior & a standard of care → median PFS/OS ∼8 mos/12 mos vs. ∼5 mos/8 mos in GEM arm (NEJM2010;362:1273)
Addition of Erlotinib to GEM + platinum doublet ↑ ORR & may ↑ PFS in CC (Lancet Onc 2012;13:181)
Concurrent chemoradiation (w/5-FU or Cap, not GEM) in select pts w/unresectable locally adv disease
Supportive care in poor performance pts