Definition (Pediatr Rev 2007;28:426)
• Serum sodium <135 mEq/L; most common electrolyte abnormality in pediatrics
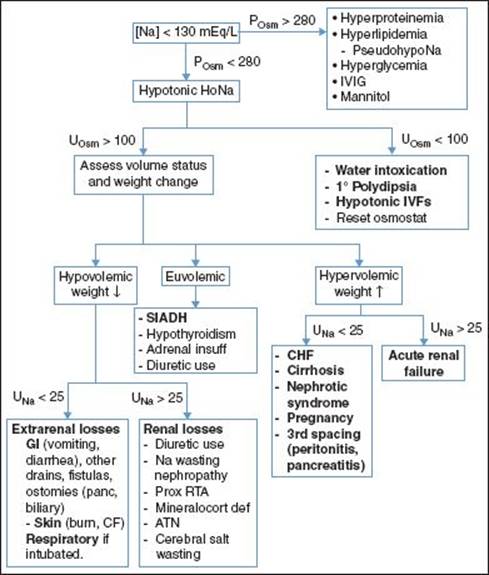
• Pseudohyponatremia is lab abnormality 2/2 ↑ serum lipid or protein (nml POsm) if gas chromatography used to assess [Na]; diff than true dilutional hyponatremia 2/2 osmotic shifts (inc POsm) 2/2 hyperglycemia, IVIG, mannitol, etc.
Pathophysiology and etiologies (Rose & Post. Clinical Physiology of Acid-Base & Electrolyte Disorders 2001:696; Peditr Clin N Am 58:1271)
• H2O excess relative to total body Na. Mech is usually impaired by renal H2O excretion; sometimes markedly excessive H2O intake (or hypotonic IVF) w/ nml excretion
• Impaired H2O excretion most often 2/2 volume loss, usually with replacement of lost volume by H2O. Other causes of impaired H2O excretion: Diuretics, channelopathies, SIADH, renal failure, ↑ collecting tubule (CT) permeability 2/2 hypothyroid or adrenal insufficiency (AI)
• Mechanism of HoNa in volume loss: ↓ volume → ↑ ADH → aquaporin channel insertion in CTs → ↑ H2O resorption
• ↓ serum Osm → H2O shift → tissue edema (esp brain); if rapid, ↑ risk herniation or apnea; if subacute or chronic, fluid shifts mitigated by loss of intracellular electrolytes (e.g., K+) and organic osmolytes
Clinical Manifestations (Pediatr Rev 2002;23:371)
• Symptoms: Neuro dysfunction 2/2 brain cell swelling (rare unless [Na] < 120 mEq/L). Even with [Na] < 120, often asymptomatic (or w/ subtle cognitive defects) if achieved slowly
• Can be nonspecific; malaise/lethargy, N/V, HA, confusion/agitation, muscle cramps, sz (2/2 pressure against rigid skull), ↓ reflexes, muscle weakness, hypothermia, irregular resp (2/2 impending herniation), coma, and even death
• Primary goal of clinical exam is assessment of volume status
Etiologies and Diagnostic Studies (Pediatr Rev 2007;28:426; Pediatr Clin N Am 2011;58:1271)
• Attempt to define chronicity
• Hx of volume loss (source), fluid repletion (type of fluid used, how formula is made, esp w/ powdered formulas), meds (diuretics, IVIG, mannitol), underlying illness (DM, hypothyroid, AI, renal channelopathy)
• Check electrolytes, serum Osm, UOsm, UNa, can check lipids and protein (pseudohypoNa)
• If hyperglycemia, hyperlipidemia, or hyperproteinemia, can correct [Na]
• Hyperglycemia: Correct up [Na] 2.4 mEq/L for each 100 mg/dL glucose above 200
• Hyperproteinemia: Correct up [Na] 0.25 × (protein [g/dL] − 8); only if Tot Prot >8
• Hyperlipidemia: Correct up [Na] 0.002 × (triglyceride [mg/dL])
• 1° polydipsia and water intoxication: 2/2 excess water intake either in 2/2 psychiatric condition w/ excess H2O consumption, or in populations unable to control intake (infants), admin of excess H2O. Rx’d w/ free water restriction
• SIADH (Am J Med 1967;42:790): Release of ADH not stim by hypovolemia or hyperosmolality (pt cannot be hypovolemic & serum Osm >275 mOsm/kg for this dx), resulting in inapprop enhanced water reabsorpt (urine Osm >100 mOsm/kg) & natriuresis
• Multiple/etiologies
• Neuro: Meningitis/encephalitis, SAH/subdural/epidural, brain abscess, stroke, neoplasm, pituitary surgery, psychosis, HIV, Guillain–Barré, TBI, SLE, MS
• Drugs: Cyclophosphamide, vincristine, vinblastine, SSRIs, antipsychotics, carbamazepine, tricyclics, MAOIs, gen anesthesia, narcotics, nicotine, desmopressin, others
• Pulmonary: PNA, TB, asthma, lung abscess, empyema, pneumothorax, PPV
• AIDS, AI, hypothyroidism
• Ectopic ADH 2/2 leukemia, lymphoma, sarcoma; small-cell lung CA (rare in peds)
Management (Rose & Post. Clinical Physiology of Acid-Base & Electrolyte Disorders 2001:696)
• Correction of HoNa is driven by patient’s symptomatology and chronicity of HoNa
• If hemodyn compromise 2/2 vol depletion, rx w/IV NS 20 cc/kg boluses until stable
• If HoNa occurred acutely, pt seizing, significant Δ MS, or impending resp arrest, then correct [Na] rapidly, otherwise slowly
• Overrapid HoNa correction (>∼12 mEq/24 hr) can result in central demyelinating lesion (particular at pons; central pontine myelinolysis) presents days to weeks after correction w/ paraparesis/quadriparesis, dysarthria, dysphagia, coma, or sz. Confirmed by CT or MRI; can take 4 wk + before radiologically detectable
• Hypovolemic HoNa: Correct HoNa by providing sodium, do not need to normalize [Na] and do not correct >12 mEq/24 hr
• Total Na deficit = (% body H2O × lean body weight[kg]) × (goal Na − measured Na)
• % body water as above; generally can use 60% (0.6) in pediatric patient
• So for 25 kg pt w/ Na 110; total Na deficit = (0.6 × 25) × (120 − 110) = 150 mEqNa
• Choose Na solution for repletion and do not replace at >12 mEq/24 hr
• If asymptomatic, replace 0.5 mEq/hr over first 24 hr
• If severe neuro sx, can replace at 1.5–2 mEq/hr for first 3–4 hr or till sx resolve, but still try not to correct >12 mEq over the first 24 hr total
• 3% NaCl has 513 mEq/L; 0.9% NaCl (NS) has 154 mEq/L
• So for above pt could give∼1 L NS over 24 hr (∼40 cc/hr), or 292 cc of 3% NaCl over 24 hr (∼12 cc/hr) for a rough correction of 0.4 mEq/L/hr, may round down to avoid over correction
• Make sure to account for insensible losses and maintenance as well
• Rough correction of severe HoNa is w/ 0.5 cc/kg/hr 3% NaCl to achieve raise in Na of 12 mEq in 24 hr. 1 cc/kg/hr to achieve in 12 hr
• Correction is never perfect, so serum [Na] should be followed q2–4h
• Hypervolemic HoNa: Generally Rx’d w/ Na and free H2O restriction, unless severe neurologic sx due to HoNa in which case replace Na as above
• Can also use diuresis (CHF and cirrhosis), or if anuric in renal failure then dialysis
• SIADH: Eliminate underlying etiology (if any); free water restriction (if needed, can use ½ maintenance or just restrict to replacement of insensible losses [40 cc/kg/d]). Isotonic IVF can make hypoNa worse if osmolarity of urine exceeds osmolarity of fluids given
• Chronic tx may include demeclocycline, lithium (contraindicated in young children), urea