Michael G. House
Presentation
A middle-aged man with a history of alcohol abuse and several previous episodes of acute pancreatitis requiring hospitalization presents with vague upper abdominal pain, weight loss, and early satiety for the past several months. Physical examination reveals a nonpulsatile fullness in the epigastrium with minimal tenderness to palpation. A serum metabolic panel is unremarkable with the exception of a recorded albumin level of 2.5 g/dL. A computed tomography (CT) scan, enhanced with intravenous contrast, is obtained and demonstrates a 6- × 8-cm fluid collection compressing the posterior wall of the gastric body (Figure 1).

FIGURE 1 • CT scan enhanced with intravenous contrast demonstrates a 6- × 8-cm fluid collection compressing the posterior wall of the gastric body
Differential Diagnosis
In the clinical setting of a patient with previous pancreatitis and a peripancreatic fluid collection, the differential diagnosis may be quite focused. Differentiation of a pancreatic pseudocyst from a peripancreatic fluid collection seen in acute pancreatitis is defined by the persistence of the lesion for 6 weeks or more from the time of the initial episode of acute pancreatitis. Other important lesions to distinguish from pancreatic pseudocysts include pancreatic mucinous cystic neoplasms (e.g., mucinous cystadenoma, intraductal papillary mucinous neoplasm), serous cystic tumors (e.g., serous cystadenoma), and visceral artery aneurysms (e.g., splenic artery aneurysm).
Workup
The mainstay of evaluation for patients with suspected chronic pancreatitis and a pancreatic pseudocyst is cross-sectional imaging. However, in addition to proper radiographic imaging, a careful evaluation of pancreatic endocrine and exocrine function should be conducted along with an overall nutritional assessment of the patient. Any clinical history of steatorrhea should be evaluated with formal fecal fat content studies. Daily fecal excretion of >7 g of fat is considered abnormal in the context of a regular balanced diet. Routine glucose monitoring and hemoglobin A1C testing can establish a diagnosis of diabetes mellitus. Patient nutritional status can be addressed globally (e.g., body mass index), but formal biochemical levels of nutritional status, including serum albumin, prealbumin, and transferrin, should be monitored.
High-resolution cross-sectional imaging with intravenous contrast, that is CT or magnetic resonance cholangiopancreatography (MRCP), will provide morphologic data on the size and structure of the pancreas, pancreatic ductal dilatation and calcifications, and the size and number of pancreatic pseudocysts (Figure 2). Relationship of the pseudocyst to the stomach, duodenum, spleen, transverse colon, and common bile duct can be addressed with either modality. Complications of pancreatitis and pseudocysts, including splenic, portal, or mesenteric vein thromboses; visceral artery pseudoaneurysms; and pseudocyst bleeding, can be identified with either CT or MRCP. Discriminating a mature pseudocyst from acute pancreatic necrosis can be difficult in some cases, particularly when the patient has suffered recurrent attacks of acute pancreatitis.

FIGURE 2 • MRCP demonstrates a large fluid collection in the region of the pancreatic head.
Distinguishing a pancreatic pseudocyst from a cystic neoplasm of the pancreas is crucial. Establishing a confident diagnosis is particularly important in patients who have no established history of pancreatitis and are being considered for nonresectional therapy (i.e., internal drainage procedures). Endoscopic ultrasound (EUS) can characterize a pancreatic pseudocyst by excluding internal septations that are frequently found in cystic neoplasms. EUS-guided fine needle aspiration of the cyst fluid can also help to discriminate these two diagnoses. Cyst fluid high in amylase but low in mucin content is consistent with a pseudocyst, whereas fluid enriched with mucin and carcinoembryonic antigen may be more suggestive of a mucinous cystic neoplasm.
Diagnosis and Treatment
Patients with symptomatic pancreatic pseudocysts should be considered for endoscopic internal drainage initially. In general, percutaneous external pseudocyst drainage is not advocated. Endoscopic retrograde cholangiopancreatography (ERCP) is helpful in determining whether a pseudocyst communicates with the main pancreatic duct and whether downstream strictures of the duct exist. Transpapillary internal drainage with stenting across the ampulla into the pseudocyst lumen is best suited for patients with mature pseudocysts containing thin fluid that communicate readily with the main pancreatic duct.
Pseudocysts that abut the posterior gastric wall can be drained internally via endoscopic cystogastrostomy. The common technique for this procedure involves puncturing the common wall with a needle knife sphincterotome, serially dilating the orifice, and placing generous transgastric double-pigtail stents to prevent spontaneous closure. Endoscopic transduodenal drainage can be accomplished in a similar manner for pseudocysts located along the head of the pancreas. Pseudocysts that contain necrotic debris may require repeated endoscopic debridements across the transgastric orifice over several weeks. Relative contraindications for endoscopic drainage include intervening perigastric varices, often observed in patients with splenic or portal vein thrombosis, and transmural distances to the pseudocyst lumen that exceed 1 cm. Operative therapy is recommended for patients who are not candidates for endoscopic drainage due to anatomic factors or those who have failed an initial endoscopic attempt.
Surgical Approach
Cholecystectomy at the time of operation should be performed for patients who harbor gallstones, even if a history of biliary pancreatitis is not established. Most pseudocysts can be drained internally into the stomach, duodenum, or small bowel. Pseudocysts located along the tail of the pancreas, and those which cannot be discriminated from cystic neoplasms, may be approached with a regional pancreatectomy, for example distal pancreatectomy. In general, proximal and central pancreatectomies are not advocated for symptomatic pseudocysts located along the head or body of the pancreas, respectively, especially when a cystic neoplasm is considered unlikely.
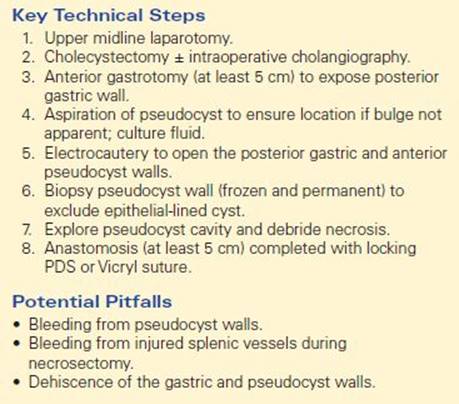
Several factors need to be considered when deciding on an appropriate operation for a symptomatic pancreatic pseudocyst. Pseudocysts that lie along the head of the pancreas and do not compress the ampulla or common bile duct can be approached with a cystoduodenostomy; however, a Roux-en-Y cystojejunostomy is often more straightforward from a technical standpoint. Pseudocysts that project through the transverse mesocolon are best managed with a Roux-en-Y cystojejunostomy with either an open or a laparoscopic technique. Cystogastrostomy is the preferred operation for pseudocysts that abut and deform the posterior gastric wall on cross-sectional imaging. An open technique is summarized in Table 1, but laparoscopic and combined laparoscopic and endoscopic techniques have been described and are being used with greater frequency in recent years. Routine placement of perianastomotic drains is not employed.
TABLE 1. Key Technical Steps and Potential Pitfalls in Open Cystogastrostomy for Pancreatic Pseudocyst
Postoperative Management
Active nutritional therapy should be considered for most patients and should be initiated soon after operation, that is, 24 to 48 hours. Enteral nutrition via a nasojejunal tube, or direct jejunostomy placed at the time of operation, is preferred over parenteral nutrition. Antibiotic therapy is discontinued after the perioperative period even for patients who were found to have a large burden of necrotic debris within the pseudocyst. Nasogastric tubes may be considered to avoid early postoperative gastric distention. A liquid diet can be introduced early in the postoperative course and advanced when appropriate.
Chronic pancreatitis is associated with thromboembolism; thus, appropriate prophylaxis for deep venous thrombosis should be carried over into the postoperative period. Morbidity after cystogastrostomy or cystojejunostomy occurs in approximately 30% of patients and includes surgical site and deep organ space infection, anastomotic bleeding, ileus, and pseudoaneurysm formation.
TAKE HOME POINTS
· Treatment of pancreatic pseudocysts should be considered for symptomatic patients.
· Pancreatic pseudocysts can become complicated by infection, bleeding, and rupture.
· EUS can help secure a diagnosis of pancreatic pseudocyst over cystic neoplasm in patients without a clear history of pancreatitis.
· MRCP and ERCP can characterize pancreatic ductal anatomy and communication with pseudocysts.
· Endoscopic internal drainage procedures are first-line therapy for patients with chronic symptomatic pseudocysts containing thin fluid.
· Surgical cystogastrostomy and cystojejunostomy are indicated for symptomatic patients who either fail or are not candidates for endoscopic drainage procedures.
· Operative procedures and techniques are selected on the basis of pseudocyst location and adjacent anatomic relationships.
SUGGESTED READINGS
Cahen D, Rauws E, Fockens P, et al. Endoscopic drainage of pancreatic pseudocysts: long-term outcome and procedural factors associated with safe and successful treatment. Endoscopy. 2005;37:977–983.
Nealon W, Walser E. Main pancreatic ductal anatomy can direct choice of modality for treating pancreatic pseudocysts. Ann Surg. 2002;235:751–758.
Schlosser W, Siech M, Beger H. Pseudocyst treatment in chronic pancreatitis: surgical treatment of the underlying disease increases long-term success. Dig Surg. 2005;22:340–345.
Sharma S, Bhargawa N, Govil A. Endoscopic management of pancreatic pseudocysts: long-term follow-up. Endoscopy. 2002;34:203–207.