Marc J. Shapiro
Steven Sandoval
Wound Classification
Surgical Site Infections
In the United States alone, an estimated 27 million surgical procedures are performed annually (1). Surgical site infections (SSIs) are the third most common nosocomial infection in most hospitalized patients accounting for 14% to 16% (Fig. 107.1). Among surgical patients, SSIs were the most common nosocomial infection, accounting for 38% of infections. Whereas 66% of the SSIs remained confined to the incision site, the remainder involved organs or spaces accessed during the surgical procedure. In 1980 it was estimated that a SSI increased hospital stay by 10 days and cost an additional $2,000 per patient (2). By 1992 that number had decreased to 7.5 days' increased stay; however, the cost had increased to $3,152 per patient. All told, the contribution to the cost of health care in the United States is calculated at 130 to 180 million dollars per year (3). The effects of SSIs are not only felt locally, such as tissue destruction, pain, scar formation, septic thrombophlebitis, but also extend systemically to septicemia, shock, organ dysfunction, and death.
Center for Disease Control (CDC) Classification of Surgical Site Infections
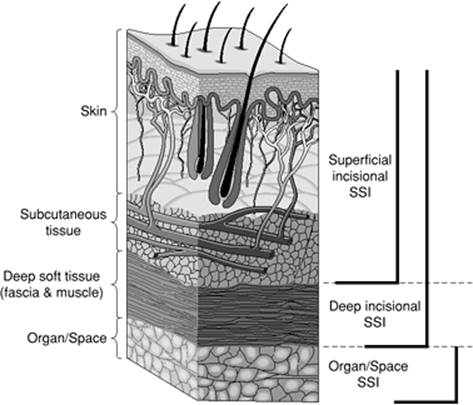
Superficial Incisional SSIs
Infection occurs within 30 days of surgery and involves only skin or subcutaneous tissue with the following:
1. Purulent drainage
2. Presence of organisms in drainage
3. Pain or tenderness, swelling, redness
Deep Incisional SSIs
Infection within 30 days of surgery, or within 1 year if implant is present. Infection involves deep soft tissues with the following:
1. Purulence from deep incision, not the organ space of operation
2. Dehiscence of deep incision or opened wound by surgeon due to symptoms of fever, pain, tenderness
3. Abscess found on direct exam or reoperation
Organ/Space SSIs
Infection within 30 days of surgery, or within 1 year if implant is present. Infection involves any part of the anatomy other than the incision opened during operation with the following:
1. Purulence from a surgically placed drain in the organ space
2. Positive cultures from that organ space
3. Abscess found on direct exam or reoperation
Purulence alone is not a hallmark of an infected wound. If purulence is present, however, a wound can be considered infected, even if confirmatory cultures are negative. The absence of confirmatory pathogens can be as a result of inadequate techniques of culture, the patient's current antimicrobial therapy, or a particularly fastidious organism. Patients with immunologic dysfunction or those who are granulocytopenic may not always produce purulent material.
Surgical wounds are grouped into four classes, each with its infection risk (Table 107.1):
· Class I (clean): An uninfected operative wound in which no inflammation is encountered and the respiratory, alimentary, genital, or uninfected urinary tract is not entered. In addition, clean wounds are primarily closed and, if necessary, drained with closed drainage. Operative incisional wounds that follow nonpenetrating (blunt) trauma should be included in this category if they meet the criteria.
· Class II (clean to contaminated): An operative wound in which the respiratory, alimentary, genital, or urinary tracts are entered under controlled conditions and without unusual contamination. Specifically, operations involving the biliary tract, appendix, vagina, and oropharynx are included in this category, provided no evidence of infection or major break in technique is encountered.
· Class III (contaminated): These include open, fresh, accidental wounds. In addition, operations with major breaks in sterile techniques (e.g., open cardiac massage) or gross spillage from the gastrointestinal tract, and incisions in which acute nonpurulent inflammation is encountered.
· Class IV (dirty to infected): Old traumatic wounds with retained devitalized tissue and those that involve existing clinical infection or perforated viscera. The organisms causing postoperative infection were present in the operative field before the operation.
Risk Factors
All surgical wounds are at risk for infection. It is important to be aware of the risk factors and if possible to take as many preventative measures as possible that will have a positive impact. The National Nosocomial Infection Surveillance (NNIS) system was developed in the early 1970s to monitor the incidence of health care–associated infections (HAIs) and their associated risk factors and pathogens. NNIS has identified wound infection risk factors as the following:
a. Wound classified as contaminated or dirty
|
|
|
Figure 107.1. Surgical site infections (SSI) categorized by depth of involvement. |
b. A patient with an ASA (American Society of Anesthesiologists) score of 3, 4, or 5 prior to operation
c. A procedure lasting longer than T hours, where T represents the 75th percentile of duration of time expected for that surgery
To identify a patient's risk index category (RIC), each factor, if present, receives a score of 1, with a range between 0 and 3. SSI rates by operative procedure category and risk index are published in NNIS source documents.
The NNIS also publishes recommendations for reducing the risk of SSIs. The weight of these recommendations are based on the scientific evidence used to support the conclusions:
1. Category IA: Strongly recommended for implementation and supported by well-designed experimental, clinical, or epidemiologic studies
2. Category IB: Strongly recommended for implementation and supported by some experimental, clinical, or epidemiologic studies and strong theoretical rationale
3. Category II: Suggested for implementation and supported by suggestive clinical or epidemiologic or theoretical rationale
4. No recommendation or unresolved issue: Practice for which insufficient evidence or no consensus regarding efficacy exists
|
Table 107.1 Surgical Wound Classification and Risk of Infection (If No Antibiotics Used) |
|||||||||||||||
|
Category IA recommendations for SSI prevention:
· Treat remote infection before performing an elective operation.
· Do not remove hair from operative sites unless it interferes with surgery and then only use electric clippers just prior to surgery.
· Select an agent with efficacy against the suspected organism, making sure the therapeutic serum levels exist from the beginning of the operation. Mechanical preparation of the colon with enemas and cathartics before elective colorectal operations and the use of nonabsorbable oral antimicrobials the day before operation have been beneficial.
Category IB recommendations for SSI prevention:
· Control serum glucose prior to operation.
· Cease tobacco use 30 days prior to operation.
· Shower night before surgery.
· Prepare operative site with an antiseptic skin agent.
· Do not routinely use vancomycin for antimicrobial prophylaxis.
· The operative team should keep nails short and not wear artificial nails.
· A 2- to 5-minute preoperative surgical scrub for the surgical team should occur.
Category II recommendations for SSI prevention:
· Prepare skin in concentric circles from the incision site outwards.
· Keep preoperative stay in the hospital as short as possible.
· Clean underneath each fingernail prior to performing first scrub of the day.
· Do not wear hand or arm jewelry.
· Limit the number of personnel entering the operating room.
No recommendation or unresolved issue: Restriction of scrub suits to the operating suite, or coverage of scrub suits outside of theater.
|
|
|
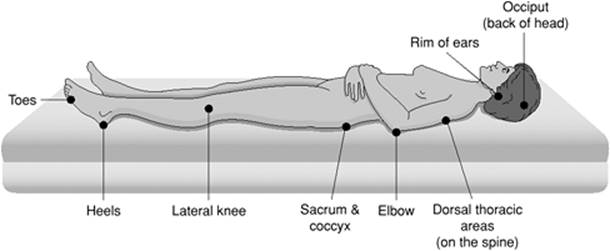
Figure 107.2. Pressure points in supine position. |
Pressure/Decubitus Ulcers
From the Latin decumbere, “to lie down,” the term decubitus has been applied to any area that develops an ulcer secondary to prolonged pressure between a bony prominence and an unyielding surface. Thus the term pressure ulcer is a more accurate description. Although an issue of long duration, it appears to be first addressed in scientific writing in the 19th century.
To overcome arterial and capillary hydrostatic pressure and develop subsequent tissue necrosis with ulceration, an individual must be subjected to 32 mm Hg pressure at the level of the ischium, sacrum, or heels for a prolonged period of time, usually exceeding 2 hours as reported by Lindan et al. (4). The points of greatest pressure with a supine patient are seen over the sacrum, heel, and occiput at 40 to 60 mm Hg (Fig. 107.2).
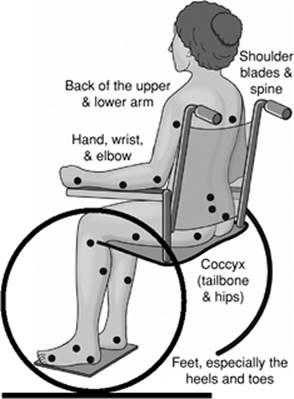
With the body in a prone position, the chest and knees absorb the greatest pressure, which may be 50 mm Hg. When the patient is sitting, the ischial tuberosities are under the most pressure, measured at near 100 mm Hg (Fig. 107.3).
|
|
|
Figure 107.3. Pressure points in sitting position. |
If sensation is intact, ulceration usually will not occur as the incipient pain would lead to a change in position by the patient. This occurs during the sleep cycle.
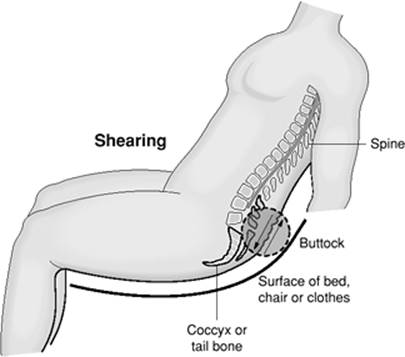
The risk factors associated with pressure ulcer development can be divided into external and internal causes. Externally, the patient might be subjected to a constant pressure for a period of time, or friction exists between exposed skin and a surface that remains static, or a region remains moist and may have desquamation, leading to a loss of the epithelial protective mechanism (Fig. 107.4). The placement of splints can also alter a patient's ability to change position in response to pressure-related pain or in itself may cause pressure necrosis. The administration of sedatives or paralytics can also remove the normal feedback pathways that exist to prevent pressure ulcer formation. Internally, factors responsible for pressure ulceration include malnutrition (serum albumin levels less than 3.0 g/dL preoperatively), anemia, and/or endothelial dysfunction. Diabetes, peripheral vascular disease, and episodes of hypotension also increase the risk as do sensory deficits in patients with plegia or paresis. Patients with dementia may also not be sensitive to the importance of changing position frequently and may also be more prone to pressure ulceration.
|
|
|
Figure 107.4. Shearing effect. |
Most patients with pressure ulcers (66%) are older than 70 years old, with a prevalence rate in nursing homes of 17% to 28%. In contrast, patients admitted with an acute illness have an incidence rate of 3% to 11%. In both subsets of patients, recurrence rates as high as 90% may be seen. The operating room, where patients are immobile is a high-risk area, and there is a report that up to 25% of all pressure ulcers are instigated there (5).
Anatomic sites affected are primarily the hip and buttocks (67% of the cases involve ischial, trochanteric, and sacral tuberosity); 25% in malleolar, heel, patellar, or pretibial area; with the remainder occurring on the nose, chin, occiput, chest, back, or elbow. In paraplegic patients, pressure ulcers are a leading cause of death, responsible for an 8% mortality rate (6). Overall an estimated 60,000 people die each year from a pressure ulcer complication. The health care cost in the United States alone per year is in excess of $1 billion (7).
Several scoring systems are used to grade the risk for ulceration. The Braden scale is a summation rating scale made up of six subscores consisting of sensory perception, moisture, activity, mobility, nutrition, and friction/shear, each ranging from 1 to 3 or 4 points, with total scores ranging from 6 to 23. The subscores measure the functional capabilities of the patient that contribute to either higher intensity and duration of pressure or lower tissue tolerance for pressure. A lower Braden score indicates lower levels of functioning with a higher risk for pressure ulcer development
The Daniels classification looks at muscle and subcutaneous tissue breakdown, which occurs before dermal and epidermal changes are observed. Epidermal necrosis occurs later because epidermal cells are able to better withstand prolonged absence of oxygen than cells in the deeper tissues both in vivo and in vitro (8). Once skin damage is visible, irreversible internal damage may have already occurred (9).
Shea staging describes ulcers that start superficially and progress to deeper structures:
· Grade I: limited to superficial epidermis and dermis
· Grade II: Involving the epidermis and dermis and extending to the adipose tissue
· Grade III: Extending through the superficial structures and adipose tissue down to muscle
· Grade IV: Complete soft tissue destruction down to bone
Currently the most widely accepted classification system for pressure ulcers is that produced by the National Pressure Ulcer Advisory Panel (NPUAP). Considered to be a modification of the Shea system, it is used only to determine initial depth, and is not a system to follow the natural history of the ulcer. It is also limited by the presence of eschar, which will mask the underlying damage. Stage I represents intact skin with signs of impending ulceration. Clinically, this may consist of blanchable erythema from reactive hyperemia that should resolve within 24 hours of relief of pressure. Warmth and induration may also be present. Continued pressure creates erythema that does not blanch. This may be the first outward sign of tissue destruction. As pressure necrosis increases, the skin may appear white from ischemia. With proper treatment, resolution should be expected in 5 to 10 days (10). Stage II represents a partial-thickness loss of skin involving epidermis and possibly dermis. This lesion may present as an abrasion, blister, or superficial ulceration, with pigmentation changes. These too represent a reversible condition. Stage III represents a full-thickness loss of skin with extension into subcutaneous tissue but not through the underlying fascia. This lesion presents as a crater with or without undermining of adjacent tissue. On examination this will appear as a necrotic, foul-smelling crater with altered light and dark pigmentation. Stage IV represents full-thickness loss of skin and subcutaneous tissue and extension into muscle, bone, tendon, or joint capsule. Osteomyelitis with bone destruction, dislocations, or pathologic fractures may be present. Sinus tracts and severe undermining commonly are present.
Treatment
All modalities of care for pressure ulcers fall along four paths:
1. Pressure reduction: Frequent turning and repositioning the patient at least every 2 hours. Historically, this was adopted because of nursing issues (it took 2 hours for the nurse to rotate all ward patients). Currently, there is debate in the literature as to this being an adequate amount of time. In addition to positioning, mattresses that reduce pressure, such as low-air-loss and air-fluidized beds should be used for patients with stage III and IV ulcers, whereas for stage I and II ulcers, the use of static mattresses such as air, foam, or water overlays are the most beneficial.
2. Wound management: Once an ulcer has developed, removal of dead tissue and debris, drainage, and protecting the surrounding healthy tissue are the goals. The pressure needed to clean wounds with no necrotic material is 2 to 5 pounds per square inch (psi). If necrotic debris is present, the pressure required increases by a factor of 2 to 3. The old wound dictum—if it is dry, wet it; if it is wet, dry it—has some validity here. A draining wound needs either a hydrocolloid or alginate, whereas a wound without drainage will respond to simple moist gauze; the surrounding skin of both need to be kept lubricated, but not wet, to reduce friction. Negative pressure therapy enhances wound healing by reducing edema, increasing the rate of granulation tissue formation, and stimulating circulation. Increased blood flow translates into a reduction in the bacterial load and delivery of infection-fighting leukocytes (11). However, there are significant contraindications for the use of vacuum-assisted or negative pressure therapy including malignancy of the wound, untreated osteomyelitis, nonenteric fistulas, and exposed vessels, organs, or nerves (12). Various dressing categories are presented in Table 107.2.
3. Surgical intervention: Debridement is the process of removing devitalized tissue. Stage III and IV ulcers will require some form of debridement, whether it is from surgical, autolytic, mechanical, or via enzymatic means. The patient's wound and overall status will dictate the means of debridement, a more stable patient receiving a more aggressive means of removing the necrotic material. In 1938, Davis (13) was the first to suggest replacing the unstable scar of a healed pressure sore with a flap of tissue. In 1947, Kostrubala and Greeley recommended excising the bony prominence and adding padding for the exposed bone with local fascia or muscle-fascia flaps. In addition, larger wounds may respond only to the placement of flaps, either fasciocutaneous or musculocutaneous. Flap failure can be seen after insufficient excision of soft tissue and bone, and if systemic factors such as nutritional status are suboptimal.
4. Nutritional support: Malnourished patients have a higher susceptibility for ulcer formation. Once formed these patients also have a diminished ability to heal or to prevent further ulcer formation in other sites. Patients with serum albumin levels less than 3 mg/dL may be candidates for supplemental feedings via enteral or parenteral routes
|
Table 107.2 Dressing Categories |
||||||||||||||
|
Primary Bacteriologic Infections
Skin and soft tissue infections are usually easily treated but have the potential of being lethal. Any break in the usual protection of the integument such as occurs with a cut, scrape, insect bite, splinter, or traumatic injury allows bacteria to enter underlying tissues. Although a scrape or a cut will not usually result in a cellulitis, a tender, firm, painful, and rapidly expanding area of redness on the skin surrounding violation of the skin barrier should be a cause for concern. Red streaks between lymph node–bearing areas may be visible, and this is indicative of a potentially spreading infection. Certain areas are more prone in becoming infected depending on the age group, such as facial cellulitis occurring more commonly in adults older than 50 years and in children 6 months to 3 years of age.
Most common causative organisms in skin infections are group A β-hemolytic streptococci and Staphylococcus aureus. Depending on the source of contamination and whether the patient is immunocompromised, Gram-negative rods and fungus can be seen. If the insult occurs during exposure to fresh water, the causative organism may be Aeromonas, a Gram-negative rod.
Predisposing states in which a minor break in the skin barrier leads to a significant infection include those patients with diabetes, immunodeficiency, varicella; venous, arterial or lymphatic insufficiency, such as that seen after lymphatic removal during mastectomy; or vein stripping for varicosities.
Treatment of uncomplicated cellulitis begins with removing the nidus of infection, cleansing the wound with an antiseptic agent, dressing the wound with an antiseptic ointment if indicated, and considering a course of oral antibiotics, such as dicloxacillin, 500 mg PO (orally) four times a day for 7 days, or cephalexin, 500 mg PO four times a day for 7 days. For patients with a suspected or known penicillin allergy, clindamycin, 400 mg, is given PO four times a day (14).
|
|
|
Figure 107.5. Erysipelas. |
Erysipelas
Erysipelas (Fig. 107.5) is a form of cellulitis that affects the epidermis primarily extending into the cutaneous lymphatics. During the Middle Ages, it was referred to as St. Anthony's fire, named after the Egyptian healer who was successful in treating this condition. It shares the same underlying cause as cellulitis with bacterial inoculation into an area of skin violation. It is more commonly seen in children and the elderly. Erysipelas differs from cellulitis in that the inflamed area is distinct from the surrounding skin, being raised and demarcated. Erysipelas is often found on the face; however, it can also develop on the arms and legs. Sometimes the skin will have what is called a peau d'orange, or orange peel, look to it. As with cellulitis, streptococcus is the primary organism identified with its toxin responsible for the brisk inflammation associated with this condition.
Treatment consists of elevation of the affected extremity, penicillin, 250 to 500 mg PO or 0.6 to 1.2 million Units intramuscularly, given every 4 to 6 hours for a 10- to 20-day course. In cases of penicillin allergy, a macrolide or cephalosporin usually suffices. If the area affected becomes ulcerated, saline dressings changed every 12 hours will assist with wound closure.
Impetigo
Also known as pyoderma, impetigo (Fig. 107.6) is the most common bacterial infection of the skin seen. It is contagious and can happen at any age but is more common in young children. Patients report skin lesions, often with associated adenopathy, with minimal systemic signs and symptoms. Impetigo may present in two forms: small vesicles with a honey-colored crust known as impetigo contagiosa, or purulent-appearing bullae, known as bullous impetigo. Most commonly caused by S. aureus, group A beta-hemolytic strep is also commonly seen in the over-2-year-old population. Warm temperatures, humidity, poor hygiene, and crowded living conditions can exacerbate the spread of impetigo. When associated with lymphadenitis in deeper infections, the term ecthyma is given. Topical mupirocin (Bactroban) applied three times a day for 5 days is successful in treating >90% of cases and is more effective than oral erythromycin (2). Lesions usually resolve completely within 7 to 10 days.
|
|
|
Figure 107.6. Impetigo due to Staphylococcus aureus in a 68-year-old diabetic who fell onto concrete while walking and developed this lesion after 6 days. This resolved with conservative care and antibiotics. |
Cutaneous Fungal Infections
The most common important fungal infections that occur in the ICU setting are for the most part due to Candida, especially albicans, glabrata, and tropicalis (2). In immunocompromised or morbidly obese patients, this usually manifests itself as cutaneous moniliasis and can be treated with topical powders or ointments. Vaginitis, of course, should be treated with suppositories, and funguria is addressed by removing or replacing the urinary catheter, which will be successful in about one third of patients.
Musculoskeletal Infections
First described in 1848, deep soft tissue infection remained a disease of unknown cause until 1920 when Meleney identified 20 patients in China in whom a hemolytic streptococcus was identified in the wounds. In Meleney gangrene, there is extensive necrosis of the skin and subcutaneous tissue caused by synergistic infection between microaerobic staphlococcal and hemolytic streptococcal infection.
|
|
||||||||||||||||||||
|
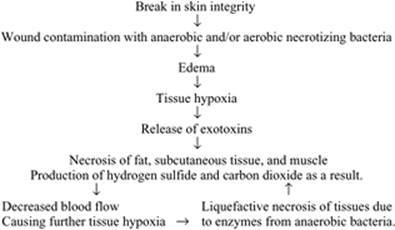
Figure 107.7. Pathophysiology of necrotizing fasciitis. |
||||||||||||||||||||
|
Table 107.3 Subtypes of Necrotizing Fasciitis (NF) |
||||||||||||||||||||
|
The term necrotizing fasciitis (NF) was first coined in 1952 by Wilson (15) and involves the underlying fascia and subcutaneous tissue and spares the muscle. Myositis results in muscle involvement, which becomes exquisitely tender and indurated. The muscle involvement leads to elevation of the creatine phosphokinase and can spread over several hours to contiguous muscle groups, thus heightening the need for early diagnosis and treatment. Fournier's gangrene is listed here as a separate entity due to its predilection for the perineum.
All of these subgroups have in common pathogenicity with the organisms spreading from subcutaneous tissues to both superficial and deep fascial planes (Figs. 107.1 and 107.7). The local effect is vascular occlusion, ischemia, and necrosis. The systemic effect is sepsis, end organ dysfunction with a mortality rate as high as 75% with Fournier's gangrene (16) and up to 100% in patients with multiple organ failure. Mortality rate varies with age and extent of involvement (17) with survivors being younger. The male:female ratio of affliction ranges 2 to 3:1.
Types of Necrotizing Fasciitis
Table 107.3 presents types of necrotizing fasciitis. Further details are discussed in the paragraphs that follow.
|
|
|
Figure 107.8. A–C: Meleney's synergistic gangrene in a 45-year-old pipe layer who noticed initially a wheal and subsequently required incision and drainage for beta-hemolytic streptococcus. |
a. Type I (polymicrobial): Usually occurring after injury or surgery, it can be misdiagnosed as a simple cellulitis; however, as tissue necrosis and hypoxia continue, pain and systemic symptoms of fever, chills, and malaise increase as the underlying tissue liquefies while the overlying skin may show minimal changes. In the late stages, extension into the muscle itself occurs. Over 2 to 3 days erythema increases, with occasional bullae formation. Cultures may reveal a combination of aerobic and anaerobic organisms. Deep soft tissue infection of the perineum is termed Fournier's gangrene (15). Many of these patients have predisposing systemic issues such as diabetes or the presence of immunosuppressed states. Histologically, thrombosis of blood vessels and abundant bacteria with many polymorphonuclear cells are typically seen.
b. Type II (group A streptococcal) (Figs. 107.8A–C and 107.9A,B): Also known familiarly as ‘flesh-eating bacteria’ or as Meleney's synergistic gangrene. As with type I, a nearly normal appearing overlying skin may result in a delay in diagnosing the underlying ongoing necrosis. A simple incision into the region affected can demonstrate drainage or even gas in advanced cases. Other predisposing factors include varicella infection and the use of nonsteroidal anti-inflammatory drugs (NSAIDs) (18). NSAID use is seen as an immunomodulator, which may predispose to this condition. With type II there is an association with the streptococcal toxic shock syndrome, similar to its staphylococcal counterpart except for the presence of necrosis as the precipitant event.
c. Type III (gas gangrene/clostridial myonecrosis): A rapidly progressive infection coined necrotizing fasciitis, it is most commonly caused by C. perfringens and less frequently by C. septicum. Most cases arise in the setting of recent surgery or trauma, being less commonly spontaneous as in types I and II. C. perfringens (formally C. welchii) is an anaerobic Gram-positive spore-forming organism that produces at least ten distinct exotoxins. The most important exotoxin leading to human pathogenesis is the alpha-toxin, which hemolyzes red blood cells, hydrolyzes cell membranes, and exerts a direct cardiodepressive effect. Within 12 to 24 hours, crepitation (Fig. 107.10) of the soft tissues may be detected by palpation (19,20). A variant of type III, known as anaerobic streptococcal myonecrosis, has a slower progression and less gas production. Aeromonas hydrophilia, a facultatively anaerobic, Gram-negative bacillus most commonly encountered in freshwater, can also yield a type III-like syndrome.
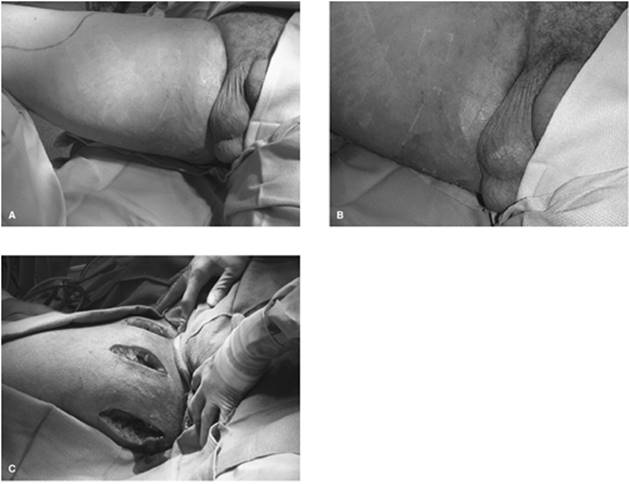
d. Fournier's gangrene (idiopathic gangrene of the penis and scrotum) (21): Although first described in 1764 by Baurienne, this entity received its name from a French venereologist, Jean-Alfred Fournier. In 1883 he presented a case of gangrene of the perineum in an otherwise healthy young man. In 95% of cases, an identifiable cause can be found, with the disease process originating from the anorectum, the urogenital tract, or the skin of the genitalia. Anorectum causes include malignancy, diverticulitis, or appendicitis. Urethral injury, urethral stricture, urogenital manipulation, or infection can initiate Fournier's gangrene, whereas cutaneous conditions like hidradenitis suppurativa or trauma can be precursors. In addition to local predisposing conditions, systemic factors such as leukemia, systemic lupus erythematosus, Crohn's disease, HIV, or other conditions of immunodeficiency may predispose one. Other predisposing comorbidities associated with Fournier's include obesity, cirrhosis, vasculitides of the perineum, steroid use, and diabetes. On exam the typical Fournier's patient will be an elderly male in his sixth or seventh decade of life with one or more of the above comorbidities. Clinically, this patient may have a history of fever and lethargy for approximately 1 week. Pain, tenderness, and erythema of the genitalia and overlying skin will progress to a dusky appearance, ultimately with purulent-appearing drainage.
|
|
|
Figure 107.9. A,B: A 25-year-old female who had a c-section 1 week prior for placenta previa and accreta who 48 hours later developed these purplish minimally raised lesions that grew out beta-hemolytic streptococcus. |
|
|
|
Figure 107.10. Necrotizing fasciitis on chest radiograph with soft tissue air in right shoulder. |
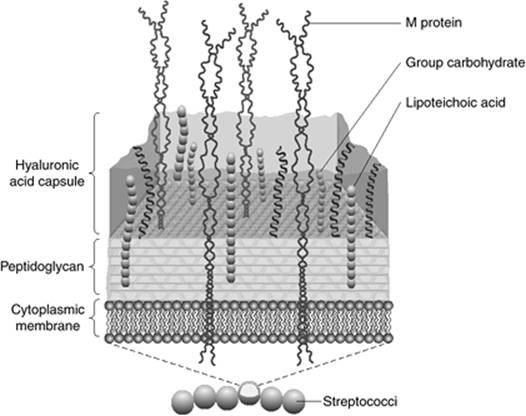
There are no predictive tests as to when a superficial infection will develop into a deep infection nor is there a chemistry test for identifying a soft tissue infection. Investigation has focused on polymerase chain reaction tests specific for streptococcal pyrogenic exotoxin (SPE) genes, variants A, B, and C along with streptococcal superantigens. These superantigens cause the release of cytokines through binding to a specific segment of the T-cell receptor, resulting in an overwhelming production of TNF-α, IL-1, and IL-6 with subsequent systemic effects of sepsis and septic shock. Work has also centered on the filamentous M-protein, which is anchored to the cell membrane and has antiphagocytic properties (Fig. 107.11).
Imaging Studies for Necrotizing Fasciitis
A summary of different imaging studies is presented in Table 107.4.
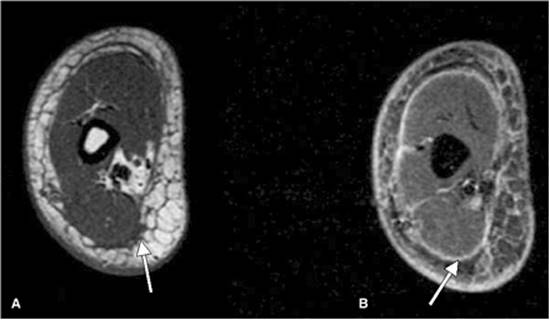
Imaging studies, in particular computerized tomography, have shown with great sensitivity the presence and extent of gas or subcutaneous air. MRI T2-weighted images (Fig. 107.12) can show well-defined areas of high signal intensity significant for tissue necrosis, and absence of gadolinium contrast enhancement on T1 images reliably detects fascial necrosis in those who might require operative debridement. Ultrasound, although able to detect fluid or gas within soft tissues, requires the probe to be applied directly on the involved tissues. Many patients with NF, especially those with Fournier's, may not tolerate this, plus there may be a limitation of the anatomic site causing difficulty in visualizing deep tissues. Yen et al. (22) found ultrasound to have a sensitivity of 88% and a specificity of 93% (positive predictive value of 83%). Their diagnostic criteria included diffuse thickening of the subcutaneous tissue accompanied by fluid accumulation more than 4 mm in depth along the fascial layer.
In addition, the diagnosis can be made with culture and biopsy of the affected tissue; a Gram stain to identify single or multiple organisms would be helpful in distinguishing type I from type II NF. Once the diagnosis is made, either on physical exam or through other diagnostic means including culture, biopsy, or excision, multimodality therapy should be used early due to the rapidity of progression.
|
|
||||||||||||||||||||
|
Figure 107.11. Action of streptococci. |
||||||||||||||||||||
|
Table 107.4 Imaging Studies |
||||||||||||||||||||
|
|
|
||||||||||
|
Figure 107.12. T1-weighted and T2-weighted magnetic resonance (MR) image of the lower extremity showing fascial thickening and fluid accumulation between the subcutaneous tissues (A) and fascial layer (B), respectively, in this patient with necrotizing fasciitis. |
||||||||||
|
Table 107.5 Clinical Indicators prompting wide surgical intervention in necrotizing fasciitis |
||||||||||
|
Therapy
Until the organism is identified, broad-spectrum antibiotics should be administered. For aerobic organisms, one regimen might be ampicillin, 8 to 14 g/day intravenously (IV) administered in every-6-hours in divided dosages, and gentamicin, 3 mg/kg per day IV divided every 8 hours. Penicillin G, 8 to 24 million Units per day IV given in divided dosages every 4 to 6 hours, should be given for presumed necrotizing fasciitis. If there is a concern of anaerobic organisms clindamycin, 600 mg IV every 6 hours, or metronidazole, not to exceed 4 g/day, can be given. In the presence of group A streptococcal infection, the use of clindamycin may be advantageous as it is not affected by inoculum size or stage of growth. Clindamycin suppresses toxin production, facilitates phagocytosis of streptococcus pyogenes by inhibiting M-protein synthesis, and suppresses production of regulatory elements controlling cell wall synthesis.
Other nonsurgical modalities include hyperbaric oxygen (HBO), although no prospective study exists to justify its value. HBO can increase the oxygen saturation in infected wounds by a thousandfold, is bacteriocidal, improves polymorphonuclear leukocytes (PMN) function, and enhances wound healing. There may be higher oxygenation and saturation in infected necrotic tissue secondary to HBO-induced vasodilation. HBO has been reported by some to improve patient survival by as much as 50% and decrease the number of debridements required to achieve wound control, whereas others have failed to show any beneficial effect (23). A typical treatment protocol involves HBO given aggressively after the first surgical debridement.
Three treatment sessions, in a multiplace chamber at 3 atmospheres absolute (ATA) at 100% oxygen for 90 minutes each, can be given in the first 24 hours; in a monoplace chamber, 2.5 to 2.8 ATA, 100% oxygen for 90 minutes per session can be given. Beginning with the second day, twice-daily treatments are given until granulation tissue is seen, usually requiring a total of 10 to 15 treatments (24). Since clostridial myonecrosis is a monobacterial anaerobic infection, hyperbaric therapy has a greater logistic role in inhibiting clostridial growth and alpha toxin production.
|
|
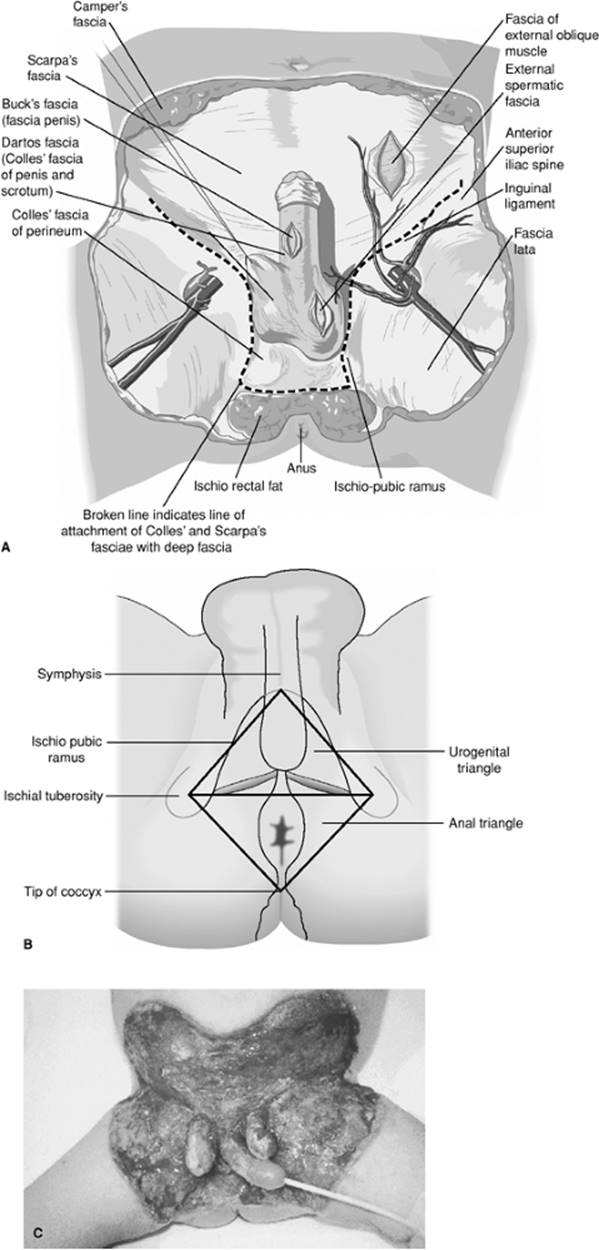
|
Figure 107.13. A-C: Fournier's gangrene involving the perineum but sparing the penis and testicles. Wide debridement has been performed. |
Intravenous immunoglobulins (IVIG) has also been used with necrotizing soft tissue infections although there are no prospective randomized trials to support its use. Case reports indicate that IVIG inhibits activation of T cells by superantigens and thereby decreases the production of TNF-α and IL-6 by T cells, providing a beneficial effect. The Canadian Streptococcal Study Group in 1998 compared 21 consecutive patients with group A streptococcal toxic shock syndrome who were administered IVIG and had a survival benefit rate of 33% (25). Several adverse side effects occurred in <5% of patients, which can mimic a worsening course of NF. Adverse effects include pallor, flushing, fever, muscle aches, hypotension, anaphylaxis, erythema multiforme, and blood-borne pathogen transmission.
Although wide local debridement may be the classical therapy for cases of necrotizing soft tissue infections (Table 107.5), initially, diagnostic surgical exploration can be limited (26,27). A series of small incisions under local anesthesia can be performed to delineate the extent and presence of muscle or facial necrosis. In addition, frozen sections of tissue specimens obtained can establish the diagnosis. However, once the diagnosis is confirmed, there exists no role for conservative debridement or incision and drainage. In the case of Fournier's gangrene, an understanding of the anatomic relationship between the perineum and abdominal wall is important. Below the area of the inguinal ligament, Scarpa's fascia blends into the Colles's fascia, which is contiguous with the dartos fascia of the penis and scrotum (Fig. 107.13A–C). This allows a potential space to exist between the Scarpa's fascia and abdominal oblique musculature, contributing to a potential spread from the perineum to the anterior abdominal wall. Due to Buck's fascia, a deep fascia that covers the corpora and anterior urethra, and due to the retroperitoneal blood supply to the testis, the penis and testicles may be spared.
The two most common pitfalls with a necrotizing soft tissue infection are diagnostic delay and inadequate debridement. Excision of nonviable areas should be early and aggressive, with repeat debridements performed until the local process has been controlled. The use of electrocautery will aid in reducing the considerable operative blood loss if the area of involvement is extensive. With perineal involvement, fecal diversion via colostomy allows for less contamination of the wound site. With urogenital involvement, continued use of a urethral catheter is safe; occasionally suprapubic cystostomy will be necessary. In the case of Fournier's gangrene, the testicles are usually spared. To prevent dessication they are usually placed in a surgically made subcutaneous pocket. If not viable, orchiectomy is performed. In all cases of NF, vacuum-assisted closure devices have shown great promise in decreasing time to grafting and closure of the debrided area (Fig. 107.9B).
Factors Associated with Poor Outcome
Factors associated with poor outcome are the following:
· Older age
· Female sex
· Elevated creatinine and lactate
· Extent of tissue involved
· Inadequate debridement
· Advanced age
· Truncal involvement
· Chest wall involvement (28)
· Presence of diabetes when in conjunction with renal dysfunction or peripheral vascular disease (29)
Summary
The major points to remember with all soft tissue and musculocutaneous infections is that aggressive and early therapy in general yields the best results. This includes local care, surgical debridement, and the use of appropriate antibiotics, which can be guided by the cultures obtained. There are many new topical products coming out on the market place which can further assist in the management of these conditions and allow for improved outcome.
References
1. Centers for Disease Control and Prevention, National Center for Health Statistics. Vital and health statistics, detailed diagnoses and procedures, national hospital discharge survey, 1994. Vol. 127. Hyattsville, MD: DHHS Publication; 1997.
2. Cruse PJ, Foord R. The epidemiology of wound infections: a 10-year prospective study of 62,939 wounds. Surg Clin North Am. 1980;60(1):27–40.
3. Martone WJ, Jarvis WR, Culver DH, et al. Incidence and nature of endemic and epidemic nosocomial infections. In: Bennett JV, Brachman PS, eds. Hospital Infections. 3rd ed. Boston, MA: Little, Brown and Company; 1992:577–596.
4. Lindan O, Greenway RM, Piazza JM. Pressure distribution on the surface of the human body. Evaluation in lying and sitting positions using a bed of springs and nails. Arch Phys Med Rehabil. 1965;46:378.
5. Up to 25% of bedsores begin in surgery: Doctor's guide. March 11, 1998. http://www.docguide.com/dg.nsf/printprint/68cbdfa3462eofdd852565c4005496d9. Accessed
6. Revis DR. Decubitus ulcers. http://www.emedicine.com/med/topic2709.htm. Accessed
7. Bennett RG, Bellantoni MF, Ouslander JG. Air-fluidized bed treatment of nursing home patients with pressure sores. J Am Geriatr Soc. 1989;37:235–242.
8. Bouten CV, Oomens CW, Baaijens FP, et al. The etiology of pressure ulcers: skin deep or muscle bound? Arch Phys Med Rehab. 2003;84:616–619.
9. Versluysen M. How elderly patients with femoral fracture develop pressure sores in the hospital. Br Med J. 1986;292:1311–1313.
10. Shea JD. Pressure sores: classification and management. Clin Orthop Rel Res. 1975;112:89–100.
11. Niezgoda JA. Combining negative pressure wound therapy with other wound management modalities. Ostomy Wound Manage. 2005;51(2A Suppl):36–38.
12. Mendez-Eastman S. Guidelines for using negative pressure wound therapy. Adv Skin Wound Care. 2001;14(6):314–22; quiz 324–325.
13. Davis JS. Operative treatment of scars following bed sores. Surgery. 1938;3:1.
14. Shapiro MJ, Smith ES, Eachempati SR. Fungal infections and antifungal therapy in the surgical intensive care unit. In: Asensio J, Trunkey D, eds. Current Therapy of Trauma and Surgical Critical Care. Philadelphia, PA: Mosby/Elsevier; 2008:702–710.
15. Wilson B. Nectrotizing Fasciitis. Am Surg. 1952;18:416.
16. Clayton MD, Fowler JE Jr, Sharifi R, et al. Causes, presentation and survival of 57 patients with necrotizing fasciitis of the male genitalia. Surg Gynecol Obstet. 1990;170:49–55.
17. Trent JT, Kirsner RS. Necrotizing fasciitis. Wounds. 2002;14(8):284–292.
18. Kaul R, McGeer A, Low DE, et al. Population-based surveillance for group A streptococcal necrotizing fasciitis: clinical features, prognostic indicators and microbiologic analysis of 77 cases. Am J Med. 1997;103:18–24.
19. Gonzalez MH. Necrotizing fasciitis and gangrene of the upper extremity. Hand Clin. 1998;14:635–645.
20. Kramer LM. Necrotizing fasciitis: a case of clostridial myonecrosis. Am J Crit Care. 2001;10(3):181–187.
21. Yanar H, Taviloglu K, Ertekin C, et al. Fournier's gangrene: risk factors and strategies for management. World J Surg. 2006;30:1750–1754.
22. Yen ZS, Wang HP, Ma HM, et al. Ultrasonographic screening of clinically suspected necrotizing fasciitis. Acad Emerg Med. 2002;9(12):1448–1451.
23. Jallali N, Withey S, Butler PE. Hyperbaric oxygen as adjuvant therapy in the management of necrotizing fasciitis. Am J Surg. 2005;189(4):462–468.
24. Korhonen K, Kuttila K, Niinikoski J. Tissue gas tensions in patients with necrotising fasciitis and healthy controls during treatment with hyperbaric oxygen: a clinical study. Eur J Surg. 2000;166(7):530–534.
25. Kaul R, McGeer A, Norrby-Teglund A. Intravenous immunoglobulin therapy for toxic shock syndrome. Clin Infect Dis. 1998;28:800–807.
26. Yong JM. Rationale for the use of intravenous immunoglobulin in streptococcal necrotizing fasciitis. Clin Immunother. 1995;4(1):61–71.
27. Urschel JD. Necrotizing soft tissue infections. Postgrad Med J. 1999;75:645–649.
28. Hammainen P, Kostiainen S. Postoperative necrotizing chest wall infections. Scand Cardiovasc J. 1998;32:243–245.
29. Elliot DC, Kufera JA, Myers RA. Necrotizing soft tissue infections: risk factors for mortality and strategies for management. Ann Surg. 1996;224:672–683.