Sherry J. Saxonhouse
William M. Miles
Jamie B. Conti
Bradyarrhythmias
Bradycardia is a common finding in hospitalized patients, especially during sleep. An increase in vagal tone may result in sinus bradycardia, sinus pauses, or atrioventricular (AV) nodal block—all physiologic findings that may have no clinical significance. Bradyarrhythmias can generally be categorized as either sinoatrial (SA) or AV conduction abnormalities.
SA Abnormalities
Sinus pauses may be caused by either sinoatrial conduction block or sinus arrest. SA conduction block occurs when impulses generated by the sinus node are not conducted to the atrial myocardium. Three categories of block are first-, second-, and third-degree SA block. First-degree SA block is not manifested on electrocardiogram, as it is merely the delay between the sinus impulse formation and atrial activation. Second-degree SA block can be type I or type II. Type I (Wenckebach) is manifested by group beating, with progressive shortening of PP intervals until a P wave is absent; this PP interval is usually less than twice the shortest cycle. Type II SA block has fixed PP intervals, followed by a pause without a P wave that is twice the PP interval (Fig. 124.1). Third-degree SA block is not visible on electrocardiogram, as no sinus impulse can escape the SA node. This disorder cannot be differentiated from sinus arrest.
Sinus arrest is the failure of automaticity in which no impulses are generated by the sinus node (Fig. 124.2). Sick sinus syndrome is dysfunction of the sinus node or SA conduction in which no adequate escape mechanism is present and the patient becomes symptomatic because of bradycardia. There are intrinsic and extrinsic causes of SA abnormalities. The most prevalent intrinsic cause of sinus node dysfunction is aging, with replacement of the sinus node and the surrounding atrium by fibrotic degeneration. Extrinsic causes of sinus node dysfunction include drugs (Table 124.1), electrolyte abnormalities (hyperkalemia), endocrine disorders (hypothyroidism), neurally mediated conditions (vasovagal syncope), and intracranial hypertension.
Diagnosis and Treatment of SA Abnormalities
1. Record a 12-lead electrocardiogram (ECG).
2. If hypotension, dizziness, and presyncope are absent, no immediate treatment is required. Symptoms dictate the treatment plan. Asymptomatic bradycardia due to sinus node dysfunction is not an emergency!
3. Evaluate the ECG for the following:
A. Myocardial infarction
B. Mechanism of bradycardia
· P-wave regularity (sinus or an atrial rhythm)
· Abrupt pauses or group beating in the sinus rhythm suggests SA block
· P waves without QRS complexes suggest AV block
· QRS axis and width for coexistent bundle branch block
4. In case of sinus bradycardia, give no treatment unless hypotension is present, then give intravenous (IV) atropine, 0.04 mg/kg of body weight.
5. In case of sinoatrial block or sinus arrest, give no treatment unless hypotension is present or the rhythm is digitalis induced (stop drug).
6. If sick sinus syndrome, then treatment depends on symptoms such as dizziness, presyncope, congestive heart failure.
7. In case of acute inferoposterior myocardial infarction (MI) with sinoatrial block, coronary reperfusion is indicated.
AV Conduction Abnormalities
AV conduction abnormalities can be categorized as first-, second-, or third-degree AV block. In first-degree AV block, every P wave is conducted to the ventricles but with a prolonged PR interval. Second-degree AV block is characterized by intermittent P waves not conducted to the ventricles and is further broken down into type I (Wenckebach), type II, and two-to-one conduction. Third-degree AV block demonstrates no conduction between the atrium and ventricles. To make the diagnosis of complete or third-degree AV block, the sinus rate must be faster than the ventricular rate.
Noninvasive Methods for Determining Site of AV Block
In AV block, the conduction abnormality may be located within the AV node, the His bundle, or the bundle branches (1). Determining the location of block is important, as this will affect immediate and long-term treatment. A 12-lead ECG and diagnostic maneuvers are helpful in diagnosing the level of block. Baseline intervals on the ECG, including PR interval, QRS duration, and axis, are important. Bedside responses to noninvasive interventions, including IV atropine administration, exercise, or vagal maneuvers, may differentiate between AV nodal and infranodal (below the AV node) block (Table 124.2). Specifically, interventions that slow AV nodal conduction, such as carotid sinus massage, will worsen AV nodal block but, because of sinus slowing, will seem to improve infranodal block. Conversely, interventions that improve AV nodal conduction, such as exercise and atropine, may worsen infranodal conduction because of acceleration of sinus rate.
|
|
|
Figure 124.1. Lead II rhythm strip. Second-degree type II sinoatrial block. The P-P interval is initially 720 ms and appears to prolong to 1,440 ms. |
First-Degree AV block or Prolonged PR Interval
The PR interval is a reflection of AV conduction time and is measured from the onset of the P wave to the beginning of the QRS complex. Conduction delay in the atrium, AV node, bundle of His, or bundle branches all may result in a prolonged PR interval. Prolongation to ≥280 ms usually indicates abnormal AV nodal conduction.
Second-Degree Type I AV Block (AV Wenckebach)
In type I AV block (Wenckebach), there is progressive lengthening of the PR interval before there is a blocked P wave (Fig. 124.3). The QRS duration may be narrow or wide, depending on the presence of bundle branch block. When the QRS is narrow, it is most likely a block occurring at the level of the AV node that will improve with atropine and exercise and worsen with carotid sinus message. It can be seen in young healthy individuals with increased vagal tone. Patients with an acute inferior myocardial infarction can have AV nodal block (≤20%), indicating a proximal right coronary occlusion (2).
Second-Degree Type II AV Block
In type II (Mobitz II) AV block, the PR intervals are normal or slightly prolonged, and are exactly the same length before and after the nonconducted P waves (Fig. 124.4). AV conduction may worsen with sinus acceleration due to atropine and exercise but may improve with carotid massage. Type II AV block is most likely infranodal in the His bundle if there is a narrow QRS duration (rare) or in the bundle branches if there is wide QRS duration (common). These patients are often symptomatic, with shortness of breath, fatigue, and syncope, and sudden progression to complete AV block.
Two-to-One AV Block
In a two-to-one AV block, every other P wave conducts to the ventricle, and the conducted PR interval may be either normal or prolonged (Fig. 124.5). The level of block—AV nodal versus infranodal—cannot be determined with certainty without an electrophysiology study. A narrow QRS duration suggests that the block is in the AV node or the His bundle whereas a wide QRS suggests block in the bundle branches.
Third-Degree AV Block or Complete AV Block
There is no P wave to QRS relationship. Sinus rate (P-to-P intervals) is usually faster than the escape rate. The escape rate is usually <50 beats per minute (bpm), with the exception of a congenital AV block (Fig. 124.6). If the escape rhythm has a narrow QRS complex, then it originates in the AV junction and the site of block is either AV nodal or, less likely, bundle of His. If the QRS is wide, the site of block is likely within the bundle branches.
|
|
|
Figure 124.2. Lead II rhythm strip. Sinus arrest with no ventricular escape. |
|
Table 124.1 Drugs Affecting Sinus Node Function |
||||||||||||
|
Diagnosis of AV Conduction Abnormalities
1. Record a 12-lead ECG and try to determine site of block by noninvasive methods.
2. In the setting of an acute inferior wall myocardial infarction (MI), the site of block is usually the AV node and is usually transient with successful reperfusion.
a. Insert a temporary pacemaker if there is cardiogenic shock secondary to heart block.
b. Use permanent pacing only if there is chronic, symptomatic second- or third-degree AV nodal block.
3. Type II AV block
a. If there is no PR prolongation prior to block, it is most likely in the His-Purkinje system.
b. Temporary pacemaker is required when associated with syncope.
c. Permanent pacemaker can be used in most cases.
4. Two-to-one AV block
a. PR interval (≤160 ms suggests His bundle or below)
b. Temporary pacemaker indicated in patients with acute MI, wide QRS, and/or if symptomatic
5. Third-degree AV block
· Temporary pacemaker required in acute anterior MI, wide QRS, and/or if symptomatic
Narrow QRS Tachycardia
Narrow QRS tachycardia is defined as an arrhythmia with a rate faster than 100 bpm and QRS duration of <120 ms. Patients are usually symptomatic, complaining of palpitations, lightheadedness, shortness of breath, or anxiety. ECG documentation of the tachycardia is extremely important to help determine the mechanism of the tachycardia. The differential diagnosis for narrow QRS tachycardia includes the following: sinus tachycardia, atrial tachycardia, atrial flutter, atrial fibrillation, AV nodal re-entry tachycardia (AVNRT), and AV re-entrant tachycardia (AVRT) using an accessory pathway.
|
Table 124.2 Noninvasive Interventions to Determine Site of Atrioventricular (AV) Block |
||||||||||||
|
Sinus tachycardia can be differentiated from other narrow QRS tachycardias by the sinus morphology of the P wave on a 12-lead ECG. Atrial fibrillation results in an irregular narrow QRS tachycardia with variable AV conduction, resulting in varying R-to-R intervals. The ventricular response to atrial flutter can be regular or irregular. The three most common causes of regular narrow QRS tachycardia are AVNRT, AVRT, and atrial tachycardia, respectively (3).
Physical examination, 12-lead ECG features during tachycardia and sinus rhythm in the same leads, and tachycardia response to carotid sinus massage will facilitate the correct diagnosis of the tachycardia. Pulsations in the neck may often reveal the mechanism of the tachycardia (Table 124.3) (4).
Atrial Tachycardia
During episodes of atrial tachycardia, an ectopic (nonsinus) P wave precedes the QRS complex. AV block can occur during tachycardia. The atrial rate is regular, with P-to-P intervals ranging between 120 and 250 bpm. The site of origin of the tachycardia within the atria can often be localized using the ECG morphology of the P wave (Fig. 124.7). Atrial tachycardias may be paroxysmal or persistent (incessant). Paroxysmal tachycardias can originate from a focal area of the myocardium or may be due to re-entry within a macrore-entrant circuit. Persistent or incessant atrial tachycardia is rare but important to recognize; patients who are in tachycardia >50% of the time may develop tachycardia-induced dilated cardiomyopathy.
Atrial Flutter
Atrial flutter typically has an atrial rate of 250 to 350 bpm. The most common form of atrial flutter uses a right atrial macrore-entrant circuit, including the cavotricuspid isthmus. Typical atrial flutter has a classic sawtooth pattern of atrial activation in the inferior leads of the ECG (Fig. 124.8). Flutter waves can be better appreciated during rapid tachycardia with slowing of the ventricular response by carotid sinus massage.
Atrial Fibrillation
Atrial fibrillation is the most common supraventricular tachyarrhythmia in the United States (5,6). It is a major cause of cardiovascular morbidity and mortality, with an increased risk of death, congestive heart failure, and stroke. The incidence of atrial fibrillation increases with age, with a lifetime risk of one in four men and women older than the age of 40 y (6). Similarly, the risk of embolic stroke from atrial fibrillation increases with age (>65 years), as well as other risk factors including hypertension, prior history of strokes, heart failure, left ventricular function of ≤35%, mitral stenosis, prosthetic heart valve, and diabetes. Therefore, stroke prevention is the key focus in the management of atrial fibrillation. Anticoagulation with warfarin, with an international normalized ratio (INR) between 2.0 and 3.0, is recommended in patients with atrial fibrillation and one or two of the above-mentioned risk factors. Recent practice guidelines have been published by Fuster et al. (7) for the management of patients with atrial fibrillation.
|
|
|
Figure 124.3. A 12-lead electrocardiogram. Sinus rhythm with type I second-degree atrioventricular conduction block. |
Atrial fibrillation can be divided into four categories: (i) new onset; (ii) paroxysmal (spontaneous termination); (iii) persistent (terminates only by pharmacologic or electrical conversion); and (iv) permanent. The atrial rhythm is irregular, with an atrial rate of 350 to 500 bpm (Fig. 124.9).
|
|
|
Figure 124.4. A 12-lead electrocardiogram. Sinus rhythm with second-degree type II atrioventricular conduction block. |
AV Nodal Re-entry Tachycardia
AV nodal re-entrant tachycardia (AVNRT) is the most common form of a regular SVT and is due to re-entry within AV nodal and perinodal tissue. The heart rhythm is regular, usually between 130 and 250 bpm. Different forms of AVNRT are classified based on the direction of the circuit and the electrophysiologic properties of the circuit. Typically, there is simultaneous activation of the atria and ventricles, with P waves either hidden or partially visible at the end of the QRS (Fig. 124.10A), producing a pseudo-r′ in V1 and pseudo-s in inferior leads during tachycardia that is not present in sinus rhythm (Fig. 124.10B, C).
|
|
|
Figure 124.5. A 12-lead electrocardiogram. Sinus rhythm with 2:1 atrioventricular conduction block with left bundle branch block suggesting block below the His bundle. |
|
|
|
Figure 124.6. A 12-lead electrocardiogram. Sinus bradycardia with third degree AV conduction block. |
|
Table 124.3 Jugular Pulsation and Supraventricular Tachycardia |
||||||||||||||||||
|
||||||||||||||||||
AV Re-entrant Tachycardia
AV re-entrant tachycardia occurs due to re-entry involving an accessory pathway, an abnormal electrical connection between the atria and ventricle (8). If the accessory pathway conducts anterogradely, certain characteristics, such as a short PR interval, broad QRS, and a delta wave typical of Wolff-Parkinson-White syndrome, may be present on surface 12-lead ECG during sinus rhythm (Fig. 124.11A). The tachycardia that results in a narrow QRS conducts anterogradely down the AV node to activate the ventricles and then conducts retrogradely up the accessory pathway to activate the atria (orthodromic AV re-entry (Fig. 124.11B); antidromic AV re-entry is discussed below. Thus, both the atria and ventricles are essential parts of the circuit. Orthodromic AV re-entry is a regular paroxysmal tachycardia, usually with the RP interval less than the PR interval (Fig. 124.11C).
|
|
|
Figure 124.7. A 12-lead electrocardiogram. Atrial tachycardia with a p wave preceding each QRS complex. The origin of the p wave is low atrial septal. |
If atrial fibrillation occurs in a patient with an anterograde-conducting accessory pathway, the impulse can conduct rapidly down the accessory pathway anterogradely, resulting in variable QRS morphologies (Fig. 124.11D). This rhythm can degenerate into ventricular fibrillation and sudden death. Treatment with intravenous ibutilide or procainamide should be first-line medical therapy for atrial fibrillation with pre-excitation, as other drug therapies can cause hypotension and further hemodynamic compromise without affecting the properties of the accessory pathway or converting to sinus rhythm.
Treatment of Regular Narrow-complex Tachycardia
1. Record 12-lead ECG during tachycardia and in sinus rhythm; record the termination of the tachycardia
2. Physical examination evaluating jugular pulse
3. Vagal maneuver; if no success, then 6 mg of rapid IV adenosine and repeat with 12 mg of IV adenosine
|
|
|
Figure 124.8. A 12-lead electrocardiogram. Atrial flutter with variable atrioventricular conduction. |
|
|
|
Figure 124.9. A 12-lead electrocardiogram. Atrial fibrillation with slow ventricular response. Note that there are no discernible p waves and that the rhythm is irregular. |
|
|
|
Figure 124.10. A: Schematic of atrioventricular (AV) nodal re-entrant tachycardia where the ventricle is passively activated. The most common form is anterograde conduction down the slow pathway and retrograde conduction up the fast pathway. B: A 12-lead electrocardiogram. Sinus rhythm of a patient with AV nodal re-entry tachycardia (AVNRT); there is no r′ in lead V1. C: A 12-lead electrocardiogram. AVNRT with pseudo r′ in lead V1 denoted by the arrow. |
|
|
|
Figure 124.11. A: A 12-lead electrocardiogram. Sinus rhythm with ventricular pre-excitation manifested as a delta wave (arrow), consistent with Wolff-Parkinson-White syndrome. B: Schematic of orthodromic atrioventricular (AV) re-entrant tachycardia with anterograde ventricular activation from the AV node and retrograde activation through an accessory pathway (AP). Next page. C: A 12-lead electrocardiogram. Narrow-complex tachycardia in the same patient was found to be AV re-entrant tachycardia with anterograde conduction down the AV node and retrograde conduction up the accessory pathway. D: A 12-lead electrocardiogram. Atrial fibrillation in a patient with anterogradely conducting accessory pathway. There are various QRS width as there is conduction simultaneously down both the AV node and the accessory pathway. This patient is at risk for ventricular fibrillation and sudden cardiac death. |
4. If tachycardia continues, then consider beta-blockers, calcium channel blockers (verapamil 5–10 mg IV, if normal left ventricular function), or digoxin
5. If tachycardia persists, use antiarrhythmic medications such as IV amiodarone, IV procainamide (10 mg/kg, no faster than 50 mg/minute), or sotalol
6. If tachycardia persists and/or patient is hemodynamically unstable, cardiovert
Treatment of Atrial Fibrillation
1. Recent onset (<48 hours) without significant heart disease and stable:
a. Pharmacologic cardioversion with flecainide (300 mg per mouth once), propafenone (600 mg per mouth), procainamide (5–10 mg/kg IV over 20 minutes), ibutilide (1 mg IV over 10 minutes, then repeat), or amiodarone (1,000 mg IV over first 24 hours)
b. Electrical cardioversion with sedation
2. Recent onset (<48 hours) and unstable: Proceed with immediate cardioversion
3. More than 48 hours and stable:
a. Control ventricular rate with beta-blockers, calcium channel blockers, and/or digoxin
b. Aspirin can be used in patients with lone atrial fibrillation (AF) (with no risk factors of heart failure, history of thromboembolism, hypertension, or diabetes)
c. Patients with risk factors should be on oral anticoagulation with warfarin, with a goal of INR of 2.0 to 3.0
d. If plan to cardiovert or treat with antiarrhythmic medications, then either anticoagulate for ≥3 weeks prior to cardioversion with therapeutic INR or use transesophageal echocardiography with cardioversion if no thrombus identified, followed by warfarin anticoagulation
4. More than 48 hours and difficulty obtaining adequate rate control: Proceed with transesophageal echocardiogram and cardioversion.
a. If no thrombus, then cardiovert and anticoagulate
b. If thrombus is present, then anticoagulate and control rate until thrombus has resolved
Wide QRS Tachycardia
There are three causes of wide-complex tachycardia: ventricular tachycardia (VT), supraventricular tachycardia (SVT) with aberrant conduction to the ventricles, or a pre-excited tachycardia. A correct and rapid diagnosis is essential, as incorrect treatment may result in hemodynamic decompensation and death (9,10).
Ventricular Tachycardia
Independent atrial and ventricular activity (AV dissociation) is an important electrocardiographic finding that is present in 60% of patients with ventricular tachycardia (Fig. 124.12). Physical examination findings of an irregular jugular pulse, known as cannon “A” waves, varying intensity of the first heart sound, and beat-to-beat changes in systolic blood pressure all are consistent with AV dissociation.
In addition, the presence of supraventricular capture beats (sinus beats that are conducted to the ventricle with a narrow QRS during a wide-complex tachycardia) or fusion beats (sinus beats that fuse with the wide-complex beat, resulting in a QRS that is narrower than the tachycardia) would be consistent with a diagnosis of ventricular tachycardia (Fig. 124.13). The wide QRS of ventricular tachycardia does not usually mimic a true bundle branch block, since in ventricular tachycardia the impulse is generated in the ventricles; therefore, careful examination of the QRS morphology can usually differentiate ventricular tachycardia from right or left bundle branch block aberrancy. In addition, if all the QRS complexes in the precordial leads V1 to V6 are negative (negative concordance), this is consistent with the diagnosis of ventricular tachycardia (Fig. 124.12). Furthermore, the wider the QRS, the more likely that tachycardia is ventricular in origin. Hemodynamic stability, age of the patient, and ventricular rate or regularity should never be used to distinguish between supraventricular or ventricular tachycardia, as they can be misleading.
|
|
|
Figure 124.12. A 12-lead electrocardiogram. Ventricular tachycardia with atrioventricular dissociation (arrows indicate p waves) and negative concordance. There is an atypical left bundle branch block pattern. |
|
|
|
Figure 124.13. A 12-lead electrocardiogram. Ventricular tachycardia with AV dissociation and fusion beats (first and second arrow) and supraventricular capture beats (third arrow) confirming the diagnosis of ventricular tachycardia. |
Supraventricular Tachycardia with Aberrancy
Supraventricular tachycardia that is aberrantly conducted still conducts down the AV node to the ventricle and can either present with a functional (intermittent) aberrancy or a fixed bundle branch block. The pattern of aberrancy is either typical left or right bundle branch block, and a baseline 12-lead ECG can determine the presence of underlying bundle branch block (Fig. 124.14A, B).
Pre-excited Tachycardia
In patients with AV accessory pathways or Wolff-Parkinson-White syndrome, wide-complex (pre-excited) tachycardias can be seen. In the antidromic AV re-entrant variety, the atrial impulse activates the ventricle anterogradely via the accessory pathway, and retrograde conduction to the atrium is through either the AV node or another accessory pathway (Fig. 124.15). Atrial tachycardias or atrial flutter can conduct via the accessory pathway to produce pre-excited tachycardias.
Treatment of Wide QRS Tachycardia
Monomorphic wide-complex tachycardia that is thought to be ventricular in origin in a stable patient can be treated with intravenous amiodarone (150 mg IV over 10 minutes; repeat as needed to a maximum dose of 2.2 grams IV per 24 hours). If amiodarone is not successful or the patient develops hemodynamic instability or symptoms, then electrical cardioversion is appropriate (11).
If the wide-complex tachycardia is thought to be SVT with aberrancy, then adenosine administration is recommended (6 mg rapid IV push followed by 12 mL of saline. If no effect, 12 mg IV push of adenosine can be tried). Adenosine may be therapeutic (terminating the tachycardia by blocking the AV node) if the patient has a re-entrant supraventricular tachycardia, or diagnostic (causing transient increase in AV block) if the patient has atrial fibrillation or flutter. In the latter case, if patient remains stable, rate-controlling intravenous drugs that have longer-lasting effects, such as beta-blockers or diltiazem, may be administered. Avoid the administration of IV verapamil if the patient has left ventricular dysfunction, heart failure, and/or if there is a possibility that the rhythm could be ventricular in origin, as verapamil has been shown to cause clinical deterioration and death (9). If the patient is hemodynamically unstable, then synchronized cardioversion is appropriate (11).
|
|
|
Figure 124.14. A: A 12-lead electrocardiogram. Atrial flutter with 1:1 conduction and typical left bundle branch block aberrancy. B: A 12-lead electrocardiogram. Atrial flutter with 2:1 conduction and typical left bundle branch block aberrancy in the same patient as in Figure 124.12A. |
|
|
|
Figure 124.15. Schematic of antidromic atrioventricular (AV) re-entry, a pre-excited tachycardia with anterograde conduction down the accessory pathway (AP) and retrograde conduction up the AV node. |
In a patient with Wolff-Parkinson-White who is in atrial fibrillation with anterograde conduction down the accessory pathway, first-line medical therapy should be intravenous procainamide, 100 mg every 5 minutes (maximum 25 to 50 mg/minute or 17 mg/kg maximum if normal renal function) or intravenous ibutilide, 1 mg over 10 minutes (may be repeated). These drugs block the rapid conduction over the accessory pathway and may also terminate the atrial fibrillation. If there is no effect, then cardiovert. If the patient is unstable, immediate cardioversion is indicated (11).
|
|
|
Figure 124.16. A 12-lead electrocardiogram. Sinus rhythm with a long QT interval (arrows indicate QT measured at approximately 520 ms). |
Drug-Induced Arrythmias
Many antiarrhythmic agents, noncardiac drugs, and nonprescription medications can cause QT prolongation (Fig. 124.16) and subsequently torsade de pointes (12). The mechanism is thought to be related to reaching the threshold potential for the slow calcium channel, resulting in early after-depolarizations and ectopic impulse formation, triggering re-entrant excitation, which results in torsade de pointes (13,14).
Torsade de Pointes
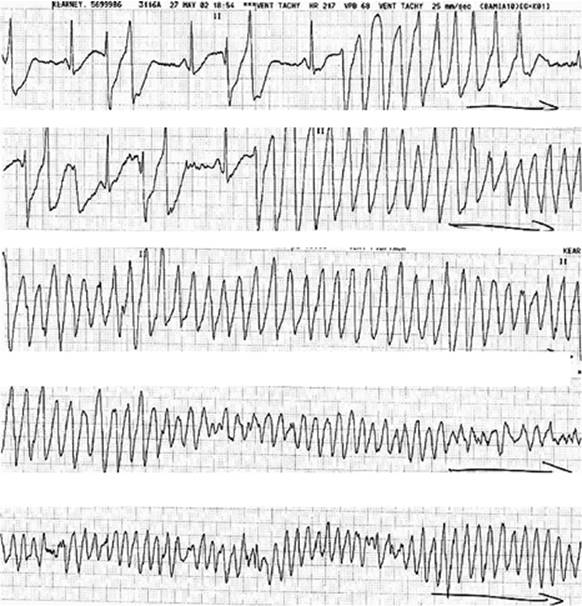
Torsade de pointes is a polymorphic VT with beat-to-beat changes in the QRS axis (Fig. 124.17); there is QT prolongation, often with a pause or bradycardia-dependent initiation of the arrhythmia. If a drug is responsible for prolonging the QT duration, it should be discontinued. The administration of IV magnesium is effective for the treatment of torsade de pointes, even when serum magnesium is normal. Hypokalemia should also be corrected. Close monitoring is essential, and if bradycardia persists, give atropine or institute temporary pacing. Isoproterenol infusion, between 1 and 4 µg/minute, can be used transiently to increase the heart rate.
Digitalis-induced Arrhythmias
Digitalis, frequently used in heart failure and atrial fibrillation, is a positive inotrope. It slows the ventricular rate during atrial fibrillation, increases vagal tone, causes diuresis, and has vasodilatory effects. Digitalis has a narrow therapeutic window, with women requiring a lower dose than men (15).
Unrecognized digitalis intoxication is a common problem and often missed by clinicians (16,17) because the symptoms of digitalis intoxication are nonspecific (gastrointestinal symptoms, visual changes, neuropsychiatric problems, and weakness), and serum drug levels do not correlate well with toxicity. It is important for any health care professional caring for patients who take digitalis to be familiar with ECG findings consistent with digitalis toxicity (17).
|
|
|
Figure 124.17. Lead II rhythm strip. Long QT interval with torsade de pointes. |
Diagnosis and Treatment
Arrhythmias due to digitalis toxicity include atrial tachycardia, junctional tachycardia, ventricular tachycardia, and bradyarrhythmias, including AV block. Many other comorbidities and conditions can potentiate digitalis toxicity, including sympathetic stimulation, hypokalemia, hypercalcemia, hypomagnesemia, diuretics, ischemia and reperfusion, and heart failure. Digitalis toxicity can manifest as four ECG features: (i) bradycardia when the heart rate was previously normal or fast; (ii) tachycardia when the heart rate was previously normal; (iii) unexpected regular rhythm when the patient previously had an irregular rhythm; and (iv) an irregular rhythm that regularly repeats itself (12).
The treatment of digitalis toxicity depends on the clinical condition and not the drug level. The first step when suspecting digitalis toxicity is to discontinue the medication. Rest, continuous ECG monitoring, and correction of electrolyte abnormalities will often help. If the arrhythmia is life threatening, administering digitalis antibodies or phenytoin may be indicated (12). The patient's kidney function must be determined to estimate the severity of the suspected intoxication.
Summary
Cardiac arrhythmias are prevalent in the intensive care setting. Once the mechanism of the arrhythmia is identified, appropriate treatment can be initiated. Bradycardia caused by sinoatrial or AV nodal conduction disorders have been outlined in this chapter. In sinus node dysfunction, symptoms should be used to guide treatment. If patients are asymptomatic, there is no need for immediate treatment; however, if the patient is symptomatic, IV atropine and/or transvenous pacing can be used.
Three degrees of AV block have been reviewed: first, second (types I and II), and third. First-degree AV block usually does not require intervention, and third-degree AV block almost always requires intervention, especially in the setting of an acute MI or heart failure. Second-degree AV block requires immediate intervention if symptomatic. The site of conduction abnormality (AV node versus His-Purkinje) in second-degree AV block can usually be determined by the pattern (type 1 or 2), the QRS width, and by noninvasive maneuvers as outlined in the chapter. In most cases, permanent pacing is required for third-degree AV block and for second-degree type II AV block.
Diagnosis and treatment of narrow and wide QRS tachycardia has also been discussed. The most common regular supraventricular tachycardia is AV nodal re-entrant tachycardia. The treatment of regular narrow-complex supraventricular tachycardia includes vagal maneuvers, IV adenosine, and IV calcium blockers or beta-blockers. Antiarrhythmic medications can be used if all others are unsuccessful as outlined above. Electrical cardioversion should be instituted as soon as the patient is hemodynamically unstable. Atrial fibrillation and atrial flutter treatment is based on the duration of the arrhythmia. If the time from onset is <48 hours, patients can be cardioverted using antiarrhythmics as outlined above, along with anticoagulation as appropriate. If the time from onset is >48 hours or unknown, rate control and anticoagulation should be instituted as outlined above, unless immediate cardioversion is necessary.
The cause of a wide-complex tachycardia should be determined quickly, as it will facilitate appropriate treatment of the patient. Various methods of differentiation have been outlined above. In general, supraventricular tachycardia with aberrancy will have a typical right or left bundle branch block pattern versus a pre-excited tachycardia or ventricular tachycardia which will not have a typical bundle branch block pattern. Differentiation between supraventricular and ventricular tachycardia can be determined with other criteria such as AV dissociation, fusion, or supraventricular capture beats as seen in ventricular tachycardia. With pre-excited tachycardia, there is usually pre-excitation (delta wave) present in sinus rhythm and a known history of Wolf-Parkinson-White.
Finally, drug-induced arrhythmias can be seen in the critical care setting. Certain drugs can prolong the QT interval and increase the risk of torsade de pointes, especially if the patient is a female and/or genetically predisposed. Other arrhythmias can be caused by digoxin toxicity, which can be potentiated by various conditions that are common in critical care patients.
Summary
Cardiac arrhythmias are common in critical care patients and may complicate the patient's clinical course. Recognition and correct diagnosis are critical for appropriate treatment to be administered. Careful evaluation of symptoms, electrocardiographic documentation of the arrhythmia, initiating and terminating factors, and response to drug administration all provide the clinician with important diagnostic information in the emergent care of these patients.
References
1. OS N. Cardiac Arrhythmias: Electrophysiology, Diagnosis, and Management. Baltimore, MD: Lippincott Williams & Wilkins; 1979.
2. Wellens HJJ, Gorgels APM, Doevendans PA. The ECG in Acute MI and Unstable Angina: Diagnosis and Risk Stratification. Boston, MA: Kluwer Academic Publishers; 2003:51.
3. Bar FW, Brugada P, Dassen WR, et al. Differential diagnosis of tachycardia with narrow QRS complex (shorter than 0.12 second). Am J Cardiol. 1984;54:555–560.
4. Harvey WP, Ronan JA Jr. Bedside diagnosis of arrhythmias. Prog Cardiovasc Dis. 1966;8:419–431.
5. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation: a major contributor to stroke in the elderly. The Framingham Study. Arch Intern Med. 1987;147:1561–1564.
6. Lloyd-Jones DM Wang TJ, Leip EP, et al. Lifetime risk for development of atrial fibrillation: The Framingham Study. Circulation. 2004;110:142–146.
7. Fuster V, Ryden LE, Cannom DS, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation. J Am Coll Cardiol. 2006;48:854–906.
8. Wellens HJJ, Brugada P, Penn OC. The management of pre-excitation syndromes. JAMA. 1987;257(17):2325–2333.
9. Buxton AE, Marchlinski FE, Doherty JU, et al. Hazards of intravenous verapamil for sustained ventricular tachycardia. Am J Cardiol. 1987;59:1107–1110.
10. Stewart RB, Bardy GH, Greene HL. Wide complex tachycardia: misdiagnosis and outcome after emergent therapy. Ann Intern Med. 1986;104:766–771.
11. Management of symptomatic bradycardia and tachycardia. Circulation. 2005;112;67–77.
12. Conover HWM. The ECG in Emergency Decision Making. Vol. 1. St. Louis, MO: Saunders Elsevier; 2006.
13. Brachmann J, Scherlag BJ, Rosenshtraukh LV, et al. Bradycardia-dependent triggered activity: relevance to drug-induced multiform ventricular tachycardia. Circulation. 1983;68:846–856.
14. Roden DM, Hoffman BF. Action potential prolongation and induction of abnormal automaticity by low quinidine concentrations in canine Purkinje fibers. Relationship to potassium and cycle length. Circ Res. 1985;56:857–867.
15. Adams KF Jr, Gheorghiade M, Uretsky BF, et al. Clinical benefits of low serum digoxin concentrations in heart failure. J Am Coll Cardiol. 2002;39:946–953.
16. Gandhi AJ, Vlasses PH, Morton DJ, et al. Economic impact of digoxin toxicity. Pharmacoeconomics. 1997;12:175–181.
17. Williamson KM, Thrasher KA, Fulton KB, et al. Digoxin toxicity: an evaluation in current clinical practice. Arch Intern Med. 1998;158:2444–2449.