Avner Sidi
Yakov Yusim
The Need
The intensive care unit (ICU) provides services for patients with life-threatening disorders. Most require analgesia and sedation for pain and anxiety management as well as mechanical ventilation, or as adjuvant therapy for bedside procedures done in the ICU (i.e., tracheostomy, venous and arterial catheterization, etc.). These patients may undergo surgical interventions outside the traditional operating room (OR) and/or “off-department” procedures such as magnetic resonance imaging (MRI) and computed tomography (CT) scan, or other radiographic examinations (1).
The roots of critical care medicine (CCM) are founded in anesthesiology, in our predecessors' efforts to extend the OR care delivered to the critically ill to the postanesthetic care unit (PACU). ICUs were developed to deal with real-time problems: Respiratory failure caused by polio epidemics in the early 1950s (2) and, later, that seen after cardiothoracic surgery (3). The needs of these high-acuity patients led to the development of better OR monitoring and more aggressive management. These devices and this approach were used not only in the OR, but also in the high-acuity areas that evolved into today's ICUs. In that regard, anesthesiology and intensive care medicine influenced and fertilized one another. This symbiosis was mostly, although not completely, positive.
Anesthesiology in Critical Care Medicine: A Continuation or Symbiosis?
As it is difficult to safely sedate the critically ill, it is not surprising that anesthetic agents moved from the OR for use in the ICU. Of course, problems may occur with long-term ICU use of drugs initially conceived for short-term OR anesthetic use (4).
Long- and Short-term Use of Anesthetic Drugs and Techniques
Pharmacotherapy
Nitrous oxide has been a key component of general anesthesia for several decades. It has also been used to provide sedation for patients in the ICU. As a result of long-term administration of nitrous oxide, a previously unseen complication developed: severe bone marrow depression due to interference with vitamin B12 metabolism (5). Similarly, when etomidate, with its excellent safety profile in the OR, was used for continuous sedation in the ICU, acute adrenal insufficiency due to impaired 11-β-hydroxylase activity was noted (6).
More recently, the difficulties with moving drugs from the OR into the ICU continue to surface. Some patients with acute respiratory distress syndrome (ARDS) require the prolonged use of neuromuscular blockers to facilitate mechanical ventilation. Ventilatory modes such as pressure control–inverse inspiration/expiration (I:E) ratio and partial liquid ventilation with perfluorocarbons all require profound sedation and, often, paralysis. When the neuromuscular blocking drugs are discontinued, patients may be profoundly weak for extended periods of time. This condition has become known as the neuromyopathy of critical illness and, while commonly reported with pancuronium, vecuronium, and other steroid-ring–based agents, it may be seen with other agents as well (7). This syndrome is prevalent in patients having received glucocorticoids during their ICU admission.
Propofol, which has many advantages over other sedative drugs in the ICU, has been associated with sepsis, which is attributed to failure to use appropriate sterile techniques with a lipid-based solution. In the pediatric and adult populations, there have been reports of fatal lactic acidosis—the propofol infusion syndrome—in association with high doses for an extended period (8,9).
Other problems can occur with the long-term use of drugs initially conceived for short-term anesthetic use. Metabolites of agents such as diazepam, midazolam, and morphine can accumulate in patients, especially the elderly or those with major organ dysfunction, resulting in prolonged sedation.
Technique: Monitoring Devices
It is not just drugs from the OR that are of interest to intensivists. The pulmonary artery catheter, initially used by cardiologists in coronary care units and coronary angiography suites in the early 1970s, was met with enthusiasm by OR anesthesiologists, especially those caring for patients during cardiac procedures. Another device developed for the OR, but of great interest in the ICU, is the bispectral index (BIS) monitor. Especially when neuromuscular blockers are used in the ICU patient for an extended period, how does one ensure that the patient is adequately sedated? Although there are few good studies documenting the utility of BIS in the ICU, increasing recognition and a possible role for such a device are evolving. Neither of these devices is without risk and controversy, although both, in our opinion, have their utility (10,11); this is discussed further in other chapters herein.
Newer Therapies in Anesthesia and the Intensive Care Unit
As clinical medicine has advanced, new syndromes have emerged. ARDS was first reported in 1967 (12), probably because before that time, patients rarely survived long enough for the full-blown syndrome to develop. Today, we have multiple organ failure/dysfunction syndrome (MODS), and it is the unusual death that results from acute hypoxia or acute hypotension.
A similar pattern is found in the OR analogues of the critically ill patient: The American Society of Anesthesiologists (ASA) physical status (PS) V patient. Although the perioperative mortality in these patients has decreased to less than 60%— both intraoperatively and in the 24 hours postoperatively—mortality occurring at greater than two weeks postoperatively during hospitalization has increased from 0% to more than 15% (13), suggesting not an actual decrease in mortality rate, but a shift in time when mortality occurs. This may also be seen in posttrauma deaths, where immediate death is related to neurologic or cardiovascular injury, or hemorrhage, and late death is due to infection, multiorgan failure, or both (14).
To a great extent, perioperative mortality is a product of the severity of illness and the advances in life support that constitute the body of the practice of anesthesiology (15). Thus, our interventions can affect the rate of acute mortality. But is mortality being decreased overall, or just postponed? In any case, to determine our priorities while practicing anesthesia in the ICU environment, we need to learn and assess patient risk and safety in the ICU.
Risk Assessment
American Society of Anesthesiologists Classification and Intensive Care Unit Patients
Assessing patient risk in the perioperative period is traditionally and routinely done using the ASA classification system. The ASA PS classification was developed in 1941 (16) and revised in 1963 (17,18) to include five categories, and modified “unofficially” and expanded in 1994 to include a sixth category for organ donors (19). Category V indicates that the “patient is moribund and not expected to survive for 24 hours with or without operation” (17,18,19). Although the ASA PS V category is associated with a high mortality, it is less clear that it is a valid predictor of death shortly after operation (13). While studies regarding morbidity and mortality in this group were published in the 1960s and 1970s (18,20,21,22,23) and in the late 1980s and 1990s (13,24,25,26,27,28,29,30,31,32,33,34,35,36,37), the original purpose of the system was only to describe the preoperative condition in order to facilitate tabulation of statistical data in anesthesiology (16). Even though the ASA PS V category predicts that a patient is at risk for death, it was never intended to be a multifactorial index or predictor of outcome (22). We have shown (12), as have others (38), that the ASA PS V category is likely not a sensitive predictor of intraoperative mortality, even though an ASA PS V status may correlate with overall perioperative mortality (18,20,21). Interestingly enough, the ASA PS score may correlate with perioperative mortality similar to or better than other systems devised to predict mortality or morbidity, such as the Goldman index in noncardiac surgery patients (39), the Reiss index in the elderly (29,30), the Hachinski Ischemic Score (HIS) in ICU patients (31), various perioperative variables (blood loss, ventilation, ICU stay) (32) or age (28,33), and in cancer patients (34). We found that the ASA PS V classification is associated with a higher incidence of untoward respiratory and cardiac events during emergency surgery (13). This finding is similar to that reported elsewhere (25,40,41). An ASA PS classification greater than 3 was found to be one of the independent predictors of severe adverse outcome associated with general anesthesia (27). Univariate analysis showed a significant correlation between ASA class and perioperative variables (intraoperative blood loss, duration of postoperative ventilation, and duration of intensive care stay), postoperative complications, and mortality rate (32) (Table 40.1).
Univariate analysis demonstrated the importance of the ASA PS classification in the development of postoperative complications in the related organ systems. Estimating the increased risk odds ratio for single variables, it was found that the risk of a complication was influenced mainly by ASA class, with ASA PS class IV having a risk odds ratio = 4.2 and ASA class III a risk odds ratio = 2.2. Thus, it is obvious that ASA physical status classification is a predictor of postoperative outcome (32).
Among ASA PS V patients, there is a high incidence of death after diagnostic procedures (13). This is probably related to the new era in both diagnostic testing and anesthetic care, such as CT and/or MRI scans of critically ill patients that involve general anesthesia or anesthesia care and monitoring during transport and the procedure. The ASA score subjectively categorizes patients into five subgroups by preoperative physical fitness. Since inception, it has been revised on several occasions and now also includes an “E” suffix denoting an emergency case (42). ASA classification makes no adjustment for age, gender, weight, or pregnancy, nor does it reflect the nature of the planned surgery, the skill of the anesthetist or surgeon, or the degree of pretheater preparation or facilities for postoperative care. While the ASA PS score does not predict risk for a particular patient or intervention—since underlying fitness is an important predictor of survival from surgery—the ASA PS score does have some correlation with outcome. As it is simple and widely understood, it is commonly used as a part of the preoperative assessment, and is an easy tool for audit.
In the United Kingdom, patients are coded according to their ASA and CEPOD (confidential enquiry into perioperative deaths) (43) scores. These describe the patient from the perspectives of basic risk banding and urgency of surgery. The scores allow anesthesiologists and surgeons to describe their workload and outcomes, which may be helpful for audit purposes and outcomes research.
Acute Physiology and Chronic Health Evaluation Score, American Society of Anesthesiologists Classification, and Other Scoring Systems
Interestingly, prediction of morbidity and mortality by the Acute Physiology and Chronic Health Evaluation (APACHE) II system, which has only up to an 85% success rate in predicting mortality (44,45), has been compared to the ASA PS score several times in the last decade. APACHE II was found to be similar to the ASA PS system in its ability to predict outcome in nonelderly patients undergoing major surgery (35); APACHE II may, however, be better in certain groups of ICU patients (31) and in elderly patients with gastrointestinal bleeding (36). Comparison of the APACHE II system to other severity classification scoring systems has been performed (44,46), and is discussed elsewhere in this textbook.
|
Table 40.1 Perioperative variables in relation to American Society of Anesthesiologists (ASA) classification |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Cardiac surgery remains a difficult area for outcome prediction in the ICU (45). A combination of intraoperative and postoperative variables, including the Parsonnet scoring system and the APACHE II and III scores, can improve predictive ability. The Parsonnet study (47) demonstrated that it is possible to design a simple method of risk stratification of open-heart surgery patients that makes it feasible to analyze operative results by risk groups and to compare results in similar groups between institutions.
Cardiac Risk and Anesthetic Risk in Intensive Care Unit Patients
Little information is available regarding the interaction of perioperative management (including ICU) and clinical outcome in patients undergoing major surgery such as cardiovascular and cardiothoracic interventions. Most data are derived from patients with ischemia undergoing aortocoronary bypass, and are extrapolated to other groups. Thirty years ago, Goldman et al. analyzed more than 1,000 patients having undergone major noncardiac surgery (48). Using multivariate analysis, they identified nine preoperative variables that independently correlated with postoperative cardiac complications. Although the patient population was “noncardiac,” the Goldman Cardiac Risk Index became popular because of the relative weight and value assigned to each factor, which facilitated calculation of “overall cardiac risk.” Eventually, this index was used to quantitate preoperative cardiac recommendations.
The scientific validity of this index has been questioned (49), as was its prediction for adverse cardiac outcome in comparison to the ASA PS classification for noncardiac surgery (50). The latter work showed that patients undergoing abdominal aortic aneurysm surgery were at higher risk for cardiac complication than suggested by the Goldman index. Another study investigated the utility of the Goldman index in vascular surgery (51), and found that more cardiac events occurred than it predicted. Thus, as a tool to plan postoperative management, the original Goldman index failed in cardiovascular patient populations.
Another prospective assessment of risk was the one conducted by Detsky et al. in patients undergoing noncardiac surgery (52,53). Changes in the index were proposed to improve its accuracy. The modified index added risk factors such as angina, pulmonary edema, and old myocardial infarction (MI), and deleted the risk factor of major surgery. Detsky et al. presented a statistical approach to assessing cardiac risk by converting average risk for patients undergoing particular surgical procedures (pretest probabilities) to average risks for patients with each index score (posttest probabilities). The likelihood ratios, presented in Table 40.2, convert a given pretest probability of complications into the posttest probability or change in risk, based on points assigned by the Detsky index. A likelihood ratio of more than 1 denotes an incremental risk over the pretest probability in a given procedure (52).
A more recent evaluation score—the Cardiac Anesthesia Risk Evaluation (CARE) score—is a simple risk classification system for cardiac surgical patients (54). It is based on clinical judgment and three clinical variables: comorbid conditions categorized as controlled or uncontrolled, surgical complexity, and urgency of the procedure (Table 40.3). This scoring system can rapidly stratify a patient for the probability of morbidity and mortality. The multifactorial risk scores of CARE were also compared to the risk indexes developed for general cardiac surgical populations in ICU patients by Parsonnet et al. (47), Tuman et al. (55), and Tu et al. (56). When the CARE score was compared to these other three multifactorial risk indexes for prediction of mortality and morbidity after cardiac surgery, the CARE score performs as well as multifactorial risk indexes for outcome prediction in cardiac surgery. Cardiac anesthesiologists use those scores in their practice and can predict patient outcome with acceptable accuracy.
|
Table 40.2 Perioperative cardiac complication ratio according to the Detsky Cardiac Risk Indexa |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
These classifications contain variables available in most of our patients and, like the CARE score, they apply to all cardiac surgical patients, and not only to those undergoing coronary artery surgery. Another system was developed in Europe by Peter and Lutz as an instrument for grading the level of anesthetic risk for a patient (57). Twenty parameters are involved in that scoring system: patient status, nature of the operation, age, weight, fasting status, consciousness, blood pressure, heart rate, pulse rate, respirations, renal function, liver function, blood glucose, electrolytes, hydration, hemoglobin, allergies, other major diseases, expected operative time, and burns (Table 40.4). Patients with a previous myocardial infarction were compared to those with no prior infarction to determine the influence of previous infarction on perioperative cardiac complications. Patients with a previous myocardial infarction had a higher perioperative myocardial infarction rate (3.8%) than did those patients with no prior history of myocardial infarction (0.4%) (57).
Although good predictive accuracy was found, there are problems. Measured ejection fraction was not included as an independent component in multifactorial risk indexes, even though evidence suggests that the degree of left ventricular (LV) dysfunction predicts outcome in noncardiac surgery (58). Thus, the cardiac risk indexes remain imperfect but useful tools for determining perioperative risk for cardiac events. Additional cardiac tests should be routinely employed in determining the individual patient's current risk status. Indeed, in an editorial, Goldman recognized that the new techniques and information changed the methods for prospective evaluation (59). The first technical breakthrough was the use of biostatistical analysis; the second used sophisticated evaluation such as echocardiography and scintigraphy to deal with the less well-defined middle-risk group. The next breakthrough may be utilization of randomized control trials—a methodologic rather than a technologic change. Work is ongoing by different investigators (60) to continuously update the cardiac risk indexes, which remain important tools in the current era.
In estimating an updated probability, it is quite possible that the risk indexes derived from a general patient population may not be accurate or perfectly applicable to more selected patient samples—such as those patients undergoing cardiac or aortic surgery, or who are in the ICU. By integrating the patient's score on a risk index with the prior probability of major complications in a large population of similar patients, the resulting “risk estimate” may be superior to the prior probability or the old risk index alone (Table 40.5).
Intensive Care Unit Procedures: Cost Savings and Patient Safety
ICU management of critically ill patients often includes anesthesia for minor procedures such as tracheostomy and percutaneous endoscopic gastrostomy (PEG) tube. Although advances in ICU airway management include percutaneous tracheostomy, semi-open tracheostomy, and conventional tracheostomy, many critically ill, surgical and injured patients still receive open tracheostomy in the OR (61). While percutaneous tracheostomy is performed routinely in many medical ICU settings, in high-risk surgical and trauma patients, often with unstable cervical spine injury and tissue edema, direct visualization of the cervical structures and trachea is imperative during tracheostomy. Open tracheostomy and PEG in the ICU can be undertaken in selected patients as part of a collaborative, multidisciplinary ICU patient management strategy (61). This is done to address the risk of patient transport, the inappropriate use of OR time, and the cost to the patient as part of an effort to standardize and improve patient care. The OR costs included basic room fee and charge per minute for general surgery and anesthesia and the anesthesia professional fee; the ICU costs included supplies. The surgical professional fee, tracheostomy tube cost, and gastroscope maintenance were not included in the analysis. For purposes of analysis, OR tracheostomy and OR PEG times were defined as 120 minutes and 60 minutes, respectively, although analysis through the fiscal year yielded widely divergent average OR times for these procedures. A cost comparison for individual procedure, total to date, and associated cost savings was shown by Knudsen et al. (61). By that comparison tracheostomy versus PEG had OR costs of $37,000 versus $17,000, ICU costs of $1,300 versus $1,700, and cost savings of $35,700 versus $15,300, respectively. Although the study is very small, tracheostomy and PEG placement in the ICU in selected patients were noted to be safe, avoided patient travel, improved OR utilization, and yielded a significant reduction in cost; in this study, there were no complications (61).
Analgesia and Sedation in the Intensive Care Unit
Principles
Sedation is an essential component in the management of intensive care patients. It is required to relieve the discomfort and anxiety caused by procedures such as tracheal intubation, ventilation, suction, and physiotherapy. It can also minimize agitation and maximize rest and appropriate sleep. Analgesia is an almost universal requirement for the intensive care patient. Adequate sedation and analgesia ameliorates the metabolic response to surgery and trauma. Too much or too little sedation and analgesia can increase morbidity.
|
Table 40.3 Cardiac Anesthesia Risk Evaluation scale (CARE score) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Sedation in the ICU varies widely, from producing complete unconsciousness and paralysis to being nursed awake, yet in comfort. There are many components to the ideal regimen, but key elements include recognition of pain, anxiolysis, amnesia, sleep, and muscle relaxation. The following are indications for sedation:
· Fear and/or anxiety
· Difficult sleeping
· Control of agitation
· Facilitation of mechanical ventilation/airway management
· Protection against myocardial ischemia
· Amnesia during neuromuscular blockade
Although the mainstay of therapy is pharmacologic, other patient needs are equally important:
· Good communication with regular reassurance from nursing staff
· Environmental control such as humidity, lighting, temperature, and noise
· Explanation prior to procedures
· Management of thirst, hunger, constipation, and full bladder
· Variety for the patient (e.g., radio, visits from relatives, washing/shaving)
· Appropriate diurnal variation—gives pattern to days
An essential goal of all critical care physicians should be to maintain an optimal level of pain control and sedation for their patients. This has become increasingly important because of evidence showing that the combined use of sedatives and analgesics may ameliorate the detrimental stress response in critically ill patients. Unfortunately, both pain and anxiety are subjective and difficult to measure, thereby limiting our ability to analyze these states and making management more challenging.
Although there is still a lack of high-quality, randomized, prospective, controlled trials that compare agents, monitoring techniques, and scoring systems, several societies have come together to publish clinical practice guidelines for sedation and analgesia. Recommended opioids are fentanyl or hydromorphone for short-term use, and morphine or hydromorphone for longer-term therapy. Midazolam or diazepam is recommended for sedation of the acutely agitated patient, while lorazepam is recommended for longer infusions. Propofol is preferred when rapid awakening is desired. The challenge for critical care physicians is to use these medications to provide comfort and safety without increasing morbidity or mortality. Most studies support the use of protocols in order to help achieve these goals. The bottom line is that most protocols end up stressing some common issues. These include, when consistent with patient safety, daily cessation of drugs to evaluate the patient and frequent reassessment of the level of sedation required by each specific patient. Much is unknown about the long-term effects of sedative and analgesic drugs used as infusions from weeks to months.
Complications from Pain and Anxiety
Undertreated pain results in many physiologic responses associated with poor outcomes (62). Stimulation of the autonomic nervous system and release of humoral factors—catecholamines, cortisol, glucagons, leukotrienes, prostaglandins, vasopressin, and β endorphins—following injury, sepsis, or surgery represent the “stress response.” This activation of the sympathetic nervous system increases heart rate, blood pressure, and myocardial oxygen consumption, which can lead to myocardial ischemia or infarction (63). An altered humoral response can lead to hypercoagulability as a result of increased level of factor VIII, fibrinogen platelet activity, and inhibition of fibrinolysis (64). Stress hormones also produce insulin resistance, increased metabolic rate, and protein catabolism. Immunosuppression is common with a noted reduction in number and function of lymphocytes and granulocytes (65). The stress response has been considered a beneficial hemostatic mechanism, but more recent data have shown that this response may be, in part, detrimental. There are data to suggest that the adequate treatment of pain can decrease the magnitude of the changes occurring following surgery, and thereby may decrease postoperative complications (66,67,68,69).
|
Table 40.4 Modification of the Anesthetic Risk Assessment, according to operation type and system functions (part A) and assessing risk categories (part B) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The ICU environment can lead to psychological difficulties. Memories of vivid nightmares, hallucinations, and paranoid delusions were prominent in studies of ICU patients after discharge (70). Patients who have been sedated and paralyzed during ventilation have reported experiencing hallucinations, delusions, and an altered sense of reality (71). Although some procedures can be explained to patients in order to relieve anxiety, not all patients requiring interventions during the acute stage of illness are in a state receptive to reasoning. These experiences result in some patients developing posttraumatic stress syndromes after their ICU stay (72). Effective therapy for anxiety and pain can reduce some of the adverse emotional experiences and decrease the incidence of postoperative neurosis (73).
|
Table 40.5 Potential use of the original multifactorial cardiac risk index to estimate the probability of cardiac complications in different types of patients |
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||
Assessment of Pain and Anxiety
Sedative/analgesic dosage of commonly used agents varies between patients. A valid method for monitoring sedation would allow sedation to be tailored to the individual. Any scoring system should be simple, easily performed, noninvasive, and, most importantly, reproducible. Physiologic variables, serum concentrations of drugs, and neurophysiologic tools such as electroencephalography (EEG), cerebral function analyzing monitor (CFAM), and lower esophageal contractility have all been used but are both expensive and unreliable. The best systems are clinically based; six levels of sedation are used:
1. Anxious and agitated
2. Cooperative, orientated, and tranquil
3. Responds to verbal commands only
4. Asleep but brisk response to loud auditory stimulus/light glabellar tap
5. Asleep but sluggish response to loud auditory stimulus/light glabellar tap
6. Asleep, no response
Evaluation of the sedation level should be completed hourly by the ICU nurse, with reduction in frequency as the patient stabilizes. It is suggested that levels 2 to 4 be considered suitable for patients in the ICU. An increase in the sedation score must prompt the physician to consider the differential diagnoses of oversedation, decreased consciousness level due to neurologic/biochemical disorder, or ICU-associated depression. It is preferable to allow the patient to breathe as soon as possible on synchronized intermittent mandatory ventilation (SIMV) or triggered ventilation, such as pressure support. Deep sedation, with or without paralysis, is reserved for severe head injury, inadequate oxygen delivery, and diseases such as tetanus.
Pain and anxiety are subject to interpretation, and are difficult to objectify and monitor from one care provider to another unless a standard is developed for assessing and monitoring these states. This is what makes management of sedation in critically ill patients one of the more challenging areas in ICU care. For pain, the most widely used scale is the visual analog scale (VAS). Patients point to a number on a horizontal line that is a representation of the spectrum of pain—from “no pain” to “the worse pain I have ever had.” The scale is simplistic and has a high degree of reliability and validity (74), but ignores other dimensions such as quantitative aspects of pain. Not all critically ill patients can use the scale because of the severity of their illnesses. Sometimes bedside nurses have to use behavioral signs such as facial expressions, movements, or posturing, or physiologic signs such as tachycardia, hypertension, or tachypnea. Unfortunately, none of these methods is exact. They depend on cultural interpretation of pain, type of illness, and use of other drugs that can alter the hemodynamic or movement parameters.
Monitoring sedation is also inexact, and a true gold standard has not been established. The Glasgow coma scale (GCS) is widely used for the assessment of level of consciousness, but validity is established only in patients with neurologic deficits. The sedation scale used most commonly worldwide is the 6-point Ramsay scale (75). The Ramsay scale is a numerical scale of motor responsiveness based on increasing depth of sedation (Table 40.6). Most comparative studies have used the Ramsay scale, but it has drawbacks. Based as it is on motor response, the scale must be modified for patients receiving muscle relaxants and, similar to pain assessment, there is no consensus as to what represents an adequate level of sedation in an individual patient. Other scales include the Sedation-Agitation Scale (SAS) (Appendix 40.1), Pain Intensity Scale (Appendix 40.1), and Motor Activity Assessment Scale (MAAS) (Table 40.7), but all have similar drawbacks.
The BIS of the EEG is known to provide information about the cortical and subcortical regions (76). The BIS scale, based on a score between 0 and 100, is an index of level of consciousness (77). It is more often used in the OR as an index of depth of anesthesia. Recently, attempts have been made to extend the use of BIS into the ICU, but preliminary reports have been conflicting because of muscle-based electrical activity or metabolic or structural abnormalities of the brain in ICU patients (78,79). More work is required to validate this technique in the ICU patient, but the theoretical benefits of a noninvasive monitor of cerebral function are self-evident. However, to date, no data have shown that BIS monitoring, when used to assess depth of sedation, significantly alters patient outcomes in the ICU (80). Because of the lack of evidence, routine use of this device was not recommended in the latest clinical practice guidelines (81).
|
Table 40.6 Ramsay's Sedation Scale |
||||||||||||||||||||
|
||||||||||||||||||||
Comparisons of Sedation Scoring Systems
As discussed above, for the assessment of sedation, several scoring systems have been introduced into clinical practice, but the differentiation of deeper sedation levels in particular remains poor. Auditory-evoked potentials (AEPs), as an objective method, were compared in assessing level of sedation to five different sedation scoring systems (Ramsay, Cohen, O'Sullivan, Armstrong, and Cook systems) (75,82,83,84,85) and studied in a prospective clinical study (86). Previous studies have shown that AEPs, especially latencies of the midlatency component Nb, could serve as an indicator of depth of anesthesia (87). Using electrophysiologic methods to evaluate sedation during ICU therapy, changes in latency of peak Nb were compared with various levels of sedation assessed by the five sedation scoring systems. As in anesthesia, latencies of Nb increased with increasing depth of sedation. Among the scoring systems, the one developed by Ramsay correlated best with changes in Nb latency (r2 = 0.68). The coefficient of determination, r2, of the other scores ranged from 0.56 to 0.61. Objective electrophysiologic monitoring is desirable during long-term sedation.
|
Table 40.7 Motor Activity Assessment Scale |
||||||||||||||||||
|
||||||||||||||||||
Sedatives Used in the Intensive Care Unit
The “ideal” sedative agent should possess the following qualities:
· Both sedative and analgesic properties
· Minimal cardiovascular side effects
· Controllable respiratory side effects
· Rapid onset/offset of action
· No accumulation in renal/hepatic dysfunction
· Inactive metabolites
· Inexpensive
· No interactions with other ICU drugs
Such a drug does not exist, and therefore, drug combinations are usually required. Sedative drugs may be given as boluses or infusions, although as a rule, infusions are preferable, with boluses utilized for procedures. Anxiety in the critically ill is best treated with a benzodiazepine, after adequate treatment of pain and correction of any reversible causes such as hypoxia, metabolic abnormalities, treatable neurologic abnormalities, infections, renal or hepatic failure, or nonclinical seizure activity (88). In recent clinical guidelines (81), the recommended choices have been narrowed to diazepam, lorazepam, midazolam, and propofol. Other drugs are haloperidol—useful for delirium—and dexmedetomidine, a new α2-receptor agonist, which is being used for ICU sedation (Table 40.8).
Benzodiazepines
These are anxiolytic, anticonvulsant, and amnesic drugs, and provide some muscle relaxation in addition to their hypnotic effect. Their effects are mediated by depressing the excitability of the limbic system via reversible binding at the γ-aminobutyric acid (GABA)–benzodiazepine receptor complex. They have minimal cardiorespiratory depressant effects, but these are synergistic with opioids. Rapid bolus doses can cause both hypotension and respiratory arrest. All benzodiazepines are metabolized in the liver. The common drugs in this class are diazepam, midazolam, and lorazepam. Overdose or accumulation can be reversed by flumazenil, the benzodiazepine receptor antagonist. It should be given in small aliquots—1 mg in 0.2-mg increments—which may be repeated once in 30 minutes, as large doses can precipitate seizures. Because of the short half-life, an infusion may be required.
|
Table 40.8 Sedatives recommended for patients in the intensive care unit |
|||||||||||||||||||||||||||||||||||
|
There is wide interpatient variability in the potency, efficacy, and pharmacokinetics of benzodiazepines, and thus, the dose must be titrated to the level of sedation. After long-term administration, the dose should be reduced gradually, or a lower dose reinstated if there are withdrawal symptoms (insomnia, anxiety, dysphoria, and sweating).
Benzodiazepines are administered intermittently (intravenous diazepam) or continuously (intravenous midazolam). The potential advantages of midazolam are its water solubility, short distribution and elimination half-lives (20 minute and 90 minute, respectively) (89), and lack of long-acting active metabolites. In contrast, diazepam has an elimination half-life of 44 hours (90) and its major active metabolite, desmethyldiazepam, has a half-life of 93 hours (91). These data are derived from a single-dose administration in normal subjects; much of midazolam's pharmacokinetic advantage is lost when administered by infusion to critically ill patients (90,92,93). In ICU patients, midazolam's elimination half-life may be greatly prolonged (91), and clinically important accumulation may occur (94). By using intermittent diazepam, there is a clinical disincentive to overdosage, as administration of each dose is a deliberate action by the bedside nurse. Continuous infusions of sedatives are more convenient, but risk oversedation if the infusion rate is not regularly reduced to test the lower limit of acceptable sedation. In terms of cost, diazepam has a clear advantage, being one-tenth the price. Although some may argue that, because of cost and the prolonged elimination half-life of midazolam in the critically ill, the standard sedative regimen should be intermittent intravenous diazepam, midazolam is more commonly used in our experience. Both regimens produced a rapid onset of acceptable sedation, but undersedation appeared more common with the less expensive diazepam regimen. Additionally, used alone, a sedation score may be an inappropriate outcome measure for a sedation trial (95).
Propofol (2, 6-Diisopropylphenol)
The mode of action of propofol is thought to be via the GABA receptor, but at a different site than the benzodiazepines. First developed as an intravenous anesthetic agent and with a rapid onset of action, it is metabolized rapidly—both hepatically and extrahepatically—and is thus ideal for continuous infusion. Recovery usually occurs within 10 minutes of discontinuation, but the agent can accumulate with prolonged use, particularly in the obese patient. It is solubilized as an emulsion, and the formulation can cause thrombophlebitis and pain, so it is ideally infused via a large or central vein. Prolonged infusions can lead to increased triglyceride and cholesterol levels and, indeed, its use is not licensed in children because of associated deaths attributable to this drug. A theoretical maximum recommended dose is thus 4 mg/kg/hour. Disadvantages also include cardiorespiratory depression, particularly in the elderly, septic, or hypovolemic patient. Infusions may color the urine green.
Ketamine
Ketamine acts at the N-methyl-D-aspartate (NMDA) receptor. In subanesthetic doses, ketamine is both a sedative and analgesic. However, it is generally not used because of the increase in blood pressure, intracranial pressure (ICP), and pulse rate that may result. It may also cause hallucinations, but these can be avoided if administered concomitantly with a benzodiazepine. It appears not to accumulate and, given its bronchodilatory properties, sometimes has a role in severe asthma. Its use in the ICU is often in conjunction with a narcotic for synergistic effect.
Etomidate
Etomidate was historically used in the ICU as an infusion, but is now no longer used in this manner. For maintenance of hypnosis, target concentration of 300 to 500 ng/mL may be achieved by administration of a two- or three-stage infusion (e.g., 100 µg/kg/minute for 10 minutes followed by 20 µg/kg/minute for 30 minutes, and then 10 µg/kg/minute), since its pharmacokinetics are described by a three-compartment model (96). It is used as a single dose (0.2–0.4 mg/kg) for induction when cardiovascular stability is desired. Some have ceased using the agent, even as a single dose, as it has been shown to cause adrenal suppression, even when used in this manner (97).
Barbiturates
Barbiturates such as Pentothal have been used in the ICU, especially in the management of patients with head injuries and seizure disorders. They cause significant cardiovascular depression and accumulate during infusions, leading to prolonged recovery times. Pentothal is still used occasionally in critically high levels of ICP to induce a “barbiturate coma” and in intractable seizure activity.
Butyrophenones and Phenothiazine
Although classified as major tranquilizers, these agents remain useful in the ICU, particularly in delirious patients. An aggressive dosing regimen of haloperidol may be particularly useful in a patient with delirium to promote calm, 2 to 10 mg IV every 10 to 15 minutes until the desired response is achieved (81). Haloperidol, in particular, causes minimal respiratory depression and has less α-blocking tendency than chlorpromazine, and hence, less hypotension. Significant side effects include prolongation of the QT interval, extrapyramidal effects, or neuroleptic malignant syndrome—and hence, haloperidol must be used with caution. Special care must be taken when using this agent with erythromycin, which may, in itself, prolong the QT interval.
Clonidine
This is the most well known of the α2 agonists, but also has α1-agonistic properties. A more specific agonist is dexmedetomidine; however, it is expensive and uncommonly available at present. It is particularly useful in patients with sympathetic overactivity such as alcohol withdrawal and tetanus, as it inhibits catecholamine release. Clonidine also is synergistic with opioids and acts at the spinal cord to inhibit nociceptive inputs, thus imparting analgesia. It is contraindicated in hypovolemia and can cause hypotension, bradycardia, and dry mouth.
Volatile Agents
Isoflurane has been used in concentrations of up to 0.6% and produces good long-term sedation, with minimal cardiorespiratory side effects and rapid awakening. Scavenging and pollution are a problem, as is incorporating the vaporizer into the ventilator. Although rarely used anymore, free fluoride ions from metabolized methoxyflurane can cause renal failure. More recently, desflurane has been shown to be effective in sedation, with rapid offset of effects.
Analgesics
Pain in the critically ill is best treated with a pure opioid agonist. The commonly available opiates all work at the µ receptors, so that the selection of the agent used should be based on pharmacokinetic characteristics. In a recent clinical guideline (81), the recommended choices have been narrowed to morphine, fentanyl, and hydromorphone. As the use of meperidine (pethidine), nonsteroidal anti-inflammatory drugs (NSAIDs), and mixed opioid agonist-antagonist agents are discouraged due to potential adverse effects, their use is not discussed. However, drugs such as morphine, a long-acting opioid that can be given parenterally or enterally, and ketamine, a sedative drug with analgesic qualities, are discussed at the end of this section because they do have specific advantages in the ICU patient, and can be used for the difficult to sedate patient. Table 40.9 lists some of the recommended drugs and their minimal suggested dosages for the treatment of pain.
|
Table 40.9 Analgesics recommended for patients in the intensive care unit |
|||||||||||||||||||||||||
|
Morphine, a long-acting opioid recommended by the consensus conference as the preferred analgesic agent for the critically ill, is the most frequently used intravenous analgesic agent in the ICU (98). Remifentanil hydrochloride is a potent µ-receptor agonist with unique features of rapid onset and rapid predictable offset of action (99), which makes it quickly adjustable to the required level of sedation. This agent may be a useful tool for sedation and analgesia in postsurgical ICU patients.
Drugs Used for Analgesia/Sedation in the Intensive Care Unit
Remifentanil
Remifentanil, an ultra-short-acting opioid metabolized by nonspecific tissue and blood esterases, has a rapid onset of action and does not accumulate after infusions even in organ dysfunction. It is, however, very expensive and can cause significant bradycardia. The efficacy and safety of a remifentanil–midazolam regimen versus a standard morphine–midazolam combination in short- and medium-term mechanically ventilated ICU subjects was recently compared (100). Remifentanil dosing was based on recommendations from a previous study evaluating remifentanil analgesia and sedation in mechanically ventilated ICU patients (101), whereas doses of morphine and midazolam were based on guidelines issued by the Society of Critical Care Medicine (98). The primary end point of the study (100) was to compare the efficacy of the two regimens, defined as the mean percentage of hours of the Sedation Agitation Scale (SAS) score (102) of 4 (Appendix 40.1). A remifentanil-based regimen was found to be more effective in providing optimal analgesia/sedation than a standard, morphine-based regimen. The remifentanil-based regimen allowed a more rapid emergence from sedation and facilitated earlier extubation. The agent is relatively expensive.
Morphine
Morphine is very commonly used and is the drug against which all other opioids are measured. The analgesic dose is highly variable, and may be delivered as an intermittent bolus—although there are problems with peak and trough effects but less accumulation—or as a continuous infusion. Morphine is primarily hepatically metabolized to two products: Morphine-3-glucuronide and morphine-6-glucuronide; both are excreted renally and may accumulate in renal dysfunction. The latter metabolite has independent, long-lasting sedative activity.
Morphine has minimal cardiovascular side effects unless given as a large bolus to hypovolemic patients or resultant from histamine release. It is relatively contraindicated in asthma and renal failure, and should be given in small increments in uncorrected hypovolemia. However, its use in renal failure is acceptable as long as the dosing interval is increased or the infusion rate reduced. Normal duration of action after a single dose is about 2 hours. As with all opioids, care should be taken in patients with hepatic failure.
Fentanyl
Fentanyl is a potent synthetic opioid derived from meperidine (pethidine). While it is considered a short-acting opioid with a rapid onset, after prolonged infusion the duration of action approaches that of morphine, although it does not accumulate in renal failure. It does not cause histamine release and is suitable for analgesia in the hemodynamically unstable patient.
Alfentanil
Alfentanil is a relatively expensive synthetic opioid with an onset of action about five times faster than fentanyl, due to the small volume of distribution, but is not as prone to accumulation as it is less lipid soluble. The duration of action is about one-third that of fentanyl and it, too, is safe in renal failure. Alfentanil has minimal cardiovascular effects and is a potent antitussive agent. Although not particularly sedating, alfentanil does possess many of the qualities desired of the ideal ICU analgesic.
Other agents include meperidine, which is not suitable for use in infusions, as the metabolite, normeperidine, may accumulate and cause convulsions. Naloxone is a specific receptor antagonist working at the OP3 (old µ) receptor; it completely abolishes the effects of all opioids at this site. The dose should be titrated slowly at the risk of unmasking arrhythmias or seizures in certain patients.
α2-Adrenoceptor Agonists
Clonidine and dexmedetomidine cause sedation, anxiolysis, and amnesia by their action at the central α2 adrenoceptors, and also have the advantages of not causing respiratory depression, in addition to their significant anesthetic-sparing effect (103). Dexmedetomidine is the newer agent, and has a greater specificity for the α2 adrenoceptor than clonidine. It has an elimination half-life of 2 hours, and is metabolized in the liver to methyl and glucuronide metabolites. Its clearance is reduced in liver failure, and it inhibits the CYP2D6 component of the enzyme cytochrome P450 (CYP) (104). Clonidine has been investigated in head-injured patients for its role in reducing catecholamine release and causing cerebral vasoconstriction, rather than as a sedative. There are conflicting studies regarding its effect on ICP, cerebral blood flow (CBF), or cerebral metabolism in head-injured patients (105).
Other Agents
Neuromuscular Blocking Agents
In some patients, muscle relaxation may be needed in addition to sedation and analgesia. It is vital to remember that neuromuscular blocking agents (NMBAs) have no effect on consciousness or comfort, and should be avoided if possible. There are no standard clinical techniques to monitor the level of consciousness in the patient receiving NMBAs, so it is necessary to give generous doses of sedative drugs. Use of NMBAs has fallen from about 90% of patients in the 1980s to 10% of patients in the 1990s in Europe and the United Kingdom (106,107,108).
Some NMBAs used in anesthesia have limited ICU use. For example, succinylcholine (suxamethonium) is used predominantly during emergency tracheal intubation, but a resultant rise in serum potassium must be expected, which makes it particularly inappropriate for use in cases of renal failure. Excessive potassium release also occurs after 48 hours in extensive burns and spinal cord injury. Pancuronium, on the other hand, is long acting, but may cause undesirable tachycardia; it may also accumulate in renal failure. Vecuronium is an analogue of the aminosteroid pancuronium, but causes minimal cardiovascular side effects. It is suitable for intubation and infusion. The dosage for intubation is 0.1 mg/kg as a bolus, while the continuous infusion is 1 to 2 µg/kg/minute as an infusion; the drug may accumulate in renal failure.
Atracurium is a benzylisoquinolinium agent metabolized by ester hydrolysis and Hoffman (spontaneous) elimination. Its metabolites are inactive and do not accumulate in renal or hepatic dysfunction. Histamine release occasionally occurs with boluses, but recovery occurs predictably within 1 hour, regardless of the duration of infusion. The intubating dose is 0.5 mg/kg, and the infusion dose is 4 to 12 µg/kg/minute.
Monitoring of NMBAs is performed using an ulnar nerve stimulator to follow the train-of-four count at the thenar eminence. Clinical monitoring such as cardiovascular reflexes to noxious stimuli should also be observed. Full “surgical” relaxation may not be necessary.
Problems with Relaxants
· The patient may be aware as a result of inadequate sedation. This can be evaluated by withdrawing muscle relaxants for a time period to allow recovery of muscular function.
· Accumulation may occur, especially with aminosteroids in acute renal failure (ARF), with prolonged paralysis after discontinuation.
· Severe myopathy and/or critical illness polyneuropathy occasionally occurs (especially with use of corticosteroids).
· There is a loss of protective reflexes.
· There is a tendency to oversedate.
· There is enhanced paralysis from other common ICU situations such as hypokalemia, aminoglycoside antibiotics, and hypophosphatemia.
The Practice: Global Practices and Practice Guidelines
As noted above, a variety of pharmacologic agents can be used for the treatment of pain and anxiety. Although recommendations have been made for sedation and analgesic regimens in the ICU, practice continues to vary widely between different ICUs. Several studies have attempted to characterize international practices by sending out surveys and questionnaires. In Europe, 63% of participants used midazolam often or always for patients requiring sedation, followed by 35% who used propofol and 9% who used haloperidol often or always for ICU patients (106). Use of narcotics was more evenly divided, with one third using morphine often or always, one third using fentanyl, and one fourth using sufentanil. Only 43% of the European ICUs used a sedation scale. When a scale was used, the Ramsay scale was used 74% of the time (106).
In Denmark, midazolam and propofol were used more frequently than diazepam (100%, 92%, and 24%, respectively) (107). For analgesia, the preferred drugs were morphine (94%), fentanyl (76%), and sufentanil (43%). Only 16% of the ICUs used a sedation scale, but they all used the Ramsay scale if one was used (107). In England, propofol was slightly more popular than midazolam, while almost no ICUs used lorazepam (108); after 72 hours of sedation, midazolam infusions are more popular. Analgesic usage included morphine, alfentanil, and fentanyl, in that order. A sedation scale was used in 67% of ICUs but, while the Ramsay scale was still the most popular, almost one third of the ICUs used another scoring system (108). Overall, although differences do exist between countries (98,109), most ICUs around the world are using similar drugs for pain and sedation. Almost all recognized the importance of adequate analgesia and anxiolysis, and very few used neuromuscular blocking agents, unless required for specific indications. The use of a sedation score seems to be gaining popularity, but a consensus as to the optimal level of sedation is lacking. Further work will be needed to see if the use of these scores can improve ICU morbidity and mortality.
|
Table 40.10 Clinical practice guidelines for sedation and analgesia from the Society of Critical Care Medicine and American College of Critical Care Medicine |
|||
|
The Society of Critical Care Medicine (SCCM) and the American College of Critical Care Medicine (ACCM), in 1995, published clinical practice guidelines for sedation and analgesia for the critically ill patient (109). These two societies have joined with the American Society of Health System Pharmacists (ASHP), and they have recently published revised clinical practice guidelines (82) (Table 40.10).
Sedation Protocols
The challenge for critical care physicians who use analgesics and sedatives is to provide patient comfort and safety without increasing morbidity and mortality. Because of the variety in practice styles, pathways to standardize patient care have attracted attention. From a mechanical ventilation standpoint, weaning protocols have been shown to improve efficiency, reduce resource utilization, improve patient outcomes, reduce overall ICU expenditures, and decrease the frequency of tracheostomies (110).
For sedation, there have been two prospective, randomized, controlled trials examining the effects of sedation protocols in the intubated patient. Brook et al. randomized 321 medical ICU patients to a nurse-implemented sedation protocol or to standard care (111). They showed that the protocol group had shorter mechanical ventilation time, length of stay, and tracheostomy rates. Kress et al. also studied medical ICU patients, but their protocol group had sedation infusions interrupted daily for a “wake-up test,” and the sedation was restarted at half the previous dose (112). The control group did not have scheduled daily decreases in the infusion rate, and care was left to the discretion of the ICU team. This group of investigators also found a statistically significant shorter duration of mechanical ventilation and length of ICU stay in the intervention group.
On the basis, in part, of the above data, recent clinical guidelines recommend that a sedation protocol be instituted and that it include daily cessation, and patient-specific targeted goals, of sedation and analgesia administration (81).
To provide the highest quality of patient care, the intensivist must constantly review treatment of sedation regimens in search of “best practice.” While randomized controlled trials (RCTs) are considered the gold standard for the evaluation of competing treatments, these have nevertheless been criticized, as strict inclusion and exclusion criteria may exclude the very patients who clinicians are obliged to treat (113). The conduct of trials in the ICU is further complicated by the varying case mix between different units so that the results of even perfectly conducted studies may not be relevant to a unit with a different case mix. As a result, it becomes necessary to develop protocols and systems for examining practice in one's own unit (95).
Daily Interruption of Sedation Protocols
Continuous sedation for patients undergoing mechanical ventilation is a double-edged sword. On the one hand, it may promote comfort and reduce agitation; on the other hand, it may prolong the duration of mechanical ventilation and interfere with assessment of neurologic status. The administration of sedative drugs by continuous infusion offers a more consistent level of sedation than intermittent bolus administration, and thus may improve patient comfort (114). Adequate sedation is often difficult to achieve with intermittent administration, and such regimens can be taxing on nurses and can hamper other aspects of patient care (115,116,117). However, a potential drawback to continuous infusions is the accumulation of the drug and the accompanying delays in the improvement of mental status. It is hypothesized that daily interruption of the sedative infusion will decrease these problems (112).
Care of critically ill patients is costly. In the United States in 1997, approximately $80.8 billion was spent on intensive care (118), and about 10% of this amount was spent on drugs (119). Ten to fifteen percent of the drug costs resulted from the purchase of sedative agents (120). Thus, a conservative estimate of the yearly cost of sedative drugs administered in intensive care units in the United States in 1997 (121) is between $0.8 billion and $1.2 billion; the cost may be higher if the use of sedative drugs increases the duration of mechanical ventilation and the length of stay in the intensive care unit.
Daily interruption of the infusion of sedative drugs shortened the duration of mechanical ventilation by more than 2 days and the length of stay in the intensive care unit by 3.5 days (112). Compared with the control group, the group assigned to daily interruption of sedation had a significantly shorter median duration of mechanical ventilation (7.3 vs. 4.9 days) and a significantly shorter median length of ICU stay (9.9 vs. 6.4 days) (112). Reducing the duration of mechanical ventilation will probably cut costs—both direct costs and those related to complications of mechanical ventilation, such as ventilator-associated pneumonia and barotrauma. Daily interruption of the sedative infusion is a practical, cost-effective intervention that can be readily performed by the nurses caring for patients in the ICU. The results of neurologic assessments can then be relayed to physicians, and infusions of sedative drugs can be restarted and adjusted as needed by the nurses. These results suggest that daily interruption of the sedative infusion provides acceptable sedation while minimizing adverse effects.
In addition, daily interruption of the sedative infusion reduced the total dose of midazolam administered by almost half (112). A trend toward using lower doses of benzodiazepines has previously been reported (122,123) and is at least partly related to the concomitant administration of opiates such as morphine. Benzodiazepines may enhance the analgesic effects of morphine (124), and this synergism may decrease the doses of benzodiazepines needed to achieve adequate sedation. In the above-mentioned study, daily interruption of the sedative infusion did not alter the doses of propofol administered (112). The concentration of propofol in plasma declines rapidly after administration is discontinued (125), which is probably why the daily period of drug stoppage in the intervention group was shorter among patients assigned to propofol than among those assigned to midazolam. Despite this difference, the patients were awake on more than 80% of days in both the intervention subgroups; this percentage did not differ according to the sedative agent used. In addition, there were no differences in the duration of mechanical ventilation or the length of stay in the intensive care unit when patients were grouped according to the sedative they received. However, the percentage of patients successfully discharged to their homes was greater in the group assigned to daily interruption of infusions than in the control group (112).
One drawback to continuous intravenous sedation is impaired mental status (126), which may prevent the early detection of neurologic dysfunction resulting from new insults. Stopping the sedative infusion for a period during each day is a simple way to improve the clinician's ability to perform daily neurologic examinations. Avoiding unnecessary diagnostic studies may reduce the rate of complications related to the transport of patients (127,128), in addition to reducing costs.
In conclusion, daily interruption of the infusion of sedative drugs is a safe and practical approach to treating patients who are mechanically ventilated. This practice decreases the duration of mechanical ventilation, ICU length of stay, and doses of benzodiazepines required. It also improves the ability of clinicians to perform daily neurologic examinations and reduces the need for diagnostic studies to evaluate unexplained alterations in mental status.
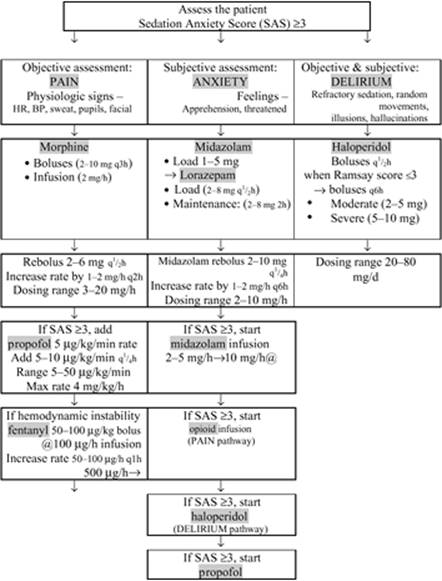
The guidelines for mechanically ventilated adults can be incorporated in three pathways: according to the level of pain, anxiety, or refractory sedation/delirium (129) (Fig. 40.1). Essential to the guidelines is the method of assessing sedation—that is, the Ramsay scale. The goal of the sedation algorithm is to maintain patients at a Ramsay score of 2 to 3. Achieving the appropriate level of sedation in a patient may be as simple as administering a midazolam bolus and a scheduled lorazepam dose, or may require the use of multiple agents. Once a patient is adequately sedated, therapy can be converted to a scheduled longer-acting lorazepam dose within 24 hours if he or she requires a midazolam or propofol infusion (Table 40.11). These guidelines use pathways that address pain and delirium, both reasons why patients often continue to be agitated and unresponsive to sedation. Midazolam and propofol are restricted to use in short-term sedation (less than 24 hours). Lorazepam can be the preferred agent for long-term sedation in critically ill patients. All patients are converted to lorazepam after 24 hours. Midazolam can still be used for loading doses in unresponsive patients receiving lorazepam or other sedatives.
Doses of Sedation Drugs
Dosing Algorithm
As mentioned above, the variety in practice styles and the pathways used to attempt to standardize patient care, choose drugs, and titrate doses can be very complicated and confusing. An example for choosing a dosing algorithm is outlined in the flow chart (Fig. 40.2) (100).
Doses of Sedation and Analgesic Drugs
The loading dose, boluses, maintenance dose, and onset and duration of common sedating and analgesic drugs are outlined in Tables 40.12 and 40.13. One can see that those doses are very similar and comparable to conscious-sedation drugs. The loading dose, maintenance dose, and plasma level of common drugs used for conscious sedation are presented in Table 40.14. The doses used in various procedures are also comparable to those used in ICU patients, and are presented in Table 40.15.
|
Table 40.11 Lorazepam conversion guide |
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
|
Figure 40.1. Guidelines for sedation and analgesia in the intensive care unit. |
||||||||||||||||||||||||||||||||||||
|
|
|
Figure 40.2. Flow chart of the study of opioid (remifentanil or morphine) and midazolam dosing algorithms. SAS, Sedation Anxiety Score. (From Dahaba AA, Grabner T, Rehak P, et al. Remifentanil versus morphine analgesia and sedation for mechanically ventilated critically ill patients: a randomized double blind study. Anesthesiology. 2004;101[3]:640–646.) |
Special Problems in Intensive Care Unit Sedation
Sedation for the Neurosurgical Patient in the Neurointensive Care Unit
Context for Use of Sedation in Head Injury
Following head injury, sedation may be instituted in emergency situations in the prehospital phase. More commonly, it is instituted in the emergency department, usually to allow for airway control. Continued use may be required in the short term (e.g., to allow an agitated patient to undergo radiologic imaging). It may also be required over the longer term in the neurointensive care unit (NICU). Sedation in the NICU is required to provide the amnesia, anxiolysis, and compliance with treatment that is required in any ICU. Additionally, it may represent an intrinsic part of the management of the head-injured patient by reduction of cerebral metabolism, with coupled reductions in cerebral blood volume (CBV) and, hence, ICP. Such agents may also be required for the control of refractory acute, posttraumatic epilepsy.
|
Table 40.12 Onset, duration, effects, and indications of common sedating drugs |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Table 40.13 The loading dose, boluses, maintenance dose, onset, and duration of common analgesic drugs |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
Properties of the Ideal Sedative Agent
The concept of the “ideal” sedative agent must be modified for use in the NICU. Traditional properties of the ideal sedative and the additional demands made by neurointensive care are specified in Table 40.16 and Figures 40.3 and 40.4. Perhaps more so than in any other critical care setting, there is a need for ease of ability to titrate agents for sedation in head injury. Such patients may require rapid increases in sedation levels to cover clinical procedures or other stimuli that could result in dangerous ICP elevations if left untreated. Other patients may require high doses of sedatives to achieve metabolic suppression.
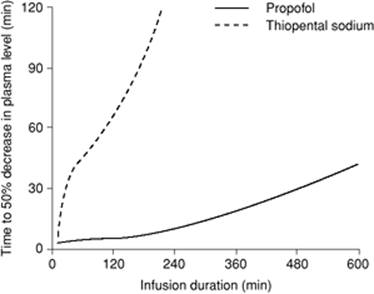
On the other hand, there may be a clinical need to achieve a rapid reversal of sedation to enable neurologic evaluation. These considerations underline the need for drugs that have not only a rapid onset, but also a rapid offset. Commonly used agents, such as sodium thiopental (thiopentone) and fentanyl, have short-lasting effects when used as a single bolus. However, cessation of drug action in these settings is achieved by rapid redistribution of the drug to a large volume of distribution (Vd), rather than by rapid drug metabolism or elimination. Repeated doses, or prolonged infusions, of such agents may saturate the Vd, and the drug effects—which are now critically dependent upon clearance rather than redistribution—may be significantly prolonged. The dependence of offset of drug effects on the duration of therapy has led to the concept of context-sensitive half-time, which takes account of the cumulative effects of drugs with prolonged administration (Fig. 40.5) (130). Thus, the most desirable agents are those with a short duration of action as a consequence of rapid excretion or metabolism—with no active metabolites—and show little or no prolongation of their duration of effect with increases in duration of administration. Even short-acting agents, such as propofol and alfentanil, may show some prolongation of effect with long-term use (Fig. 40.6). Perhaps the only current agent that seems substantially immune to this phenomenon is remifentanil (Fig. 40.6, Table 40.17) (131).
|
Table 40.14 Dosages of drugs for conscious sedation |
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Table 40.15 Intravenous bolus sedation technique |
||||||||||||||||
|
||||||||||||||||
|
Table 40.16 Characteristics of an ideal sedative used on the neurointensive care unit |
||||||||||||||||
|
||||||||||||||||
Pattern of Sedative Use
Many different sedatives have been used over the years in the NICU. A survey of sedative use in the United Kingdom and Ireland in 1995 showed the frequency of use of different sedative and analgesic agents in neurointensive care units (132,133). Most centers used a combination of a hypnotic and an opioid, the usual agents being propofol (65%), midazolam (80%), morphine (60%), fentanyl (46%), and alfentanil (26%). None of these agents is ideal, and there are few published studies that compare sedative drugs either within or between the different pharmacologic subclasses. See Table 40.17 for a summary of the main classes of sedatives.
To conclude, there is no ideal sedative for use in head injury, and few studies directly compare the effectiveness and adverse effects of different agents in this group of patients. Among the existing drugs, propofol appears to have most of the properties required but, as with all commonly used agents, it is at the expense of systemic blood pressure. The other frequently used agents, such as opioids and benzodiazepines, also have features to recommend them. In the absence of new, improved drugs, sedation of head-injured patients will likely continue to involve a number of agents. The introduction of remifentanil is promising, with its unique metabolic pathway allowing intense narcosis with a rapid and reliable offset of action, and the potential neuroprotective action of dexmedetomidine is worthy of further study.
Sedation in the Thermally Injured Patient
The quality and intensity of pain in severely burned patients during ICU treatment frequently changes due to repeated operations and dressing changes. Adequate analgesia is crucial in the critical care of burn victims, and not only to increase patient comfort, although this is of obvious concern. Either administration of too much or too little analgesia can worsen outcome: Pain decreases wound healing and immunologic competence, while overdosage of analgesics decreases intestinal motility and increases the length of stay in the ICU. The optimal concept of analgesia, following the World Health Organization (WHO) guidelines for pain management, should therefore consist of sufficient basic pain relief combined with a fast-onset “rescue” medication that provides on-top (additive) analgesia if needed (134). The combination of a NSAID and a long-acting opioid (morphine hydrochloride) with the short-acting esterase-metabolized opioid remifentanil on top seemed to be a promising concept for burn patients. The experience with this new concept of analgesia in severely burned ICU patients, with burn wounds of 20% to 80% total body surface area (TBSA), has been detailed (134). These patients received 75 mg diclofenac twice daily with a continuous IV infusion of morphine; a remifentanil infusion was added on demand if necessary. Morphine was administered in a mean dosage of 4 mg/hour. Remifentanil was administered at a median dosage of 0.7 mg/hour. This method of treatment allowed adequate individual analgesia according to actual demand, without serious side effects in severely burned patients. It can be used in both intubated and spontaneously breathing, nonintubated patients. Additionally, a cost analysis showed benefits compared to a conventional regimen (134).
|
|
|
Figure 40.3. Desirable organ-specific effects, of the ideal sedative agent, used in intensive care unit patients with brain injury. Several organ systems may be compromised by extracranial injury, making the patient more susceptible to unwanted effects of sedative agents. |
Analgesia and Sedation following Cardiac Surgery
Maintaining homeostasis after heart surgery is central to the patient's outcome. Pain and anxiety are factors contributing to postoperative morbidity, since they correlate with elevated heart rate and blood pressure, increased peripheral O2 consumption, and elevated serum adrenergic neurohormone levels.
Multiple drug combinations can be administered in the cardiac ICU. In a trial to identify the most adequate drug for the postoperative ICU setting, a prospective, randomized, open-label study was performed (135). This study's aim was a comparative analysis of a central adrenergic α2 blocker, dexmedetomidine, versus a short-acting opioid, remifentanil, with regard to analgesia, sedation, and side effects. Both drugs proved effective for controlling pain and anxiety. Remifentanil was more efficient in this study, especially when time was not considered, based on the better results in the first 4 hours of the postoperative period.
Short-acting Drugs for Long-term Intensive Care Unit Sedation
Inhalational Intensive Care Unit Sedation
ICU sedation poses many problems. The action and side effects of intravenous drugs in the severely ill patient population of an ICU are difficult to control. The incidence of posttraumatic stress disorder (PTSD) after long-term sedation is high. The recent focus on propofol infusion syndrome entails restrictions in the use of this drug. On the other hand, volatile anesthetics very selectively suppress consciousness but leave many autonomic functions intact. In the absence of perception, processing the number of adverse experiences should be lower, leading to a better psychological outcome. Respiration and intestinal motility are not depressed, facilitating modern therapeutic modalities such as early enteral feeding and augmentation of spontaneous breathing. Awakening after inhalational ICU sedation is quick and predictable; extubation can be planned and organized, and the time during which the patient needs very close observation will be short (136).
|
|
|
Figure 40.4. Schematic diagram showing the effect of different sedative agents on cerebral metabolism (CMRO2) and coupled cerebral blood flow (CBF). The diagram demonstrates the “ceiling” effect on these parameters of benzodiazepines and opioids. Barbiturates and other anesthetics, in different doses, will reduce metabolism to a point where the electroencephalogram (EEG) is isoelectric and metabolism has been reduced to basal levels. (From Urwin SC, Menon DK. Review article: comparative tolerability of sedative agents in head-injured adults. Drug Saf. 2004;27[2]:107–133.) |
Technologic advances have greatly simplified the application of inhalational anesthetics. New anesthesia ventilators offer ventilatory modes and high-flow generation comparable to ICU ventilators; however, they are not yet licensed for stand-alone use. The introduction of a volatile anesthetic reflection filter for the first time enables “inhalational sedation” to be performed with very little effort in many ICUs. This “anesthetic conserving device” (AnaConDa) is connected between the patient and a normal ICU ventilator, and retains 90% of the volatile anesthetic inside the patient, exactly like a heat and moisture exchanger. The possible advantages of the new modality and the choice of the inhalational agent are still under discussion (136).
|
|
|
Figure 40.5. Schematic diagram showing the context-sensitive half-times for thiopental sodium and propofol. Note that the recovery characteristics of both drugs worsen with increasing duration of administration, but that this effect is much more prominent for thiopental sodium. (From Urwin SC, Menon DK. Review article: comparative tolerability of sedative agents in head-injured adults. Drug Saf. 2004;27[2]:107–133.) |
|
|
|
Figure 40.6. Schematic diagram showing the context-sensitive half-times for different opioids. Unlike the other agents, remifentanil has constant recovery characteristics irrespective of duration of administration. (From Urwin SC, Menon DK. Review article: comparative tolerability of sedative agents in head-injured adults. Drug Saf. 2004;27[2]:107–133.) |
Briefly, the AnaConDa (ACD) is a modified heat and moisture exchanger (HME) with a bacterial filter, which incorporates an extra layer of activated carbon. The anesthetic is supplied in a liquid form via a syringe pump to a porous rod evaporator, which diffuses the anesthetic over a large surface. The anesthetic is instantaneously dragged and vaporized inside the ACD by the inspiratory gas flow and delivered to the lungs. The activated carbon layer absorbs some of the expired anesthetic vapor and desorbs some of it in the next inspiration (137). In this way, it can be used as a vaporizer device with a standard critical care ventilator, saving anesthetic loss like a low-flow circle anesthetic system. In fact, it has proved to reduce anesthetic consumption to a level equivalent to that produced in a circle system using a fresh gas flow of 1.5 L (138). Figure 40.7 shows the main components of ACD (139).
Bedside Anesthesia in the Intensive Care Unit
Principles of Procedural Anesthesia at the Bedside
Prospective planning requires knowledge of the patient's condition and an assessment of the anesthetic requirements of the proposed procedure. The spectrum of anesthetic options ranges from sedation and analgesia and monitored anesthesia care (MAC) to total intravenous anesthesia (TIVA) (138).
Procedural anesthesia at the bedside offers patients relief from anxiety, discomfort, and pain, and may expedite the procedure by increasing patient cooperation. Identification of the at-risk patient and modifying the anesthetic should reduce complications (see Risk Assessment section). The choice of pharmaceuticals (see above) depends upon the level of anticipated required anesthesia. Personnel requirements also vary. Although an anesthesiologist is not required to administer medications and monitor the patient for sedation and analgesia or monitored anesthesia care, TIVA does require the services of an anesthesiologist. Costs are influenced by the personnel requirements and length of the procedure, which sets the drug requirements and drug costs. In the end, personal experience combined with knowledge should guide the provider to offer efficacious and cost-effective procedural anesthesia in the ICU.
|
Table 40.17 Main sedative agents used in the treatment of head-injured patients in the neurointensive care unit |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Figure 40.7. A: Anesthetic converting device, AnaConDa. B: Breathing circuit with anesthetic converting device (AnaConDa) at the inspiratory limb of the breathing circuit. (From Sackey PV, Martling CR, Radell PJ. Three cases of PICU sedation with isoflurane delivered by AnaConDa. Paediatr Anaesth. 2005;15[10]:879–885.) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Inhalational Anesthetic Agents: The Nonresponding Patient
Halothane, isoflurane, and sevoflurane are potent bronchodilators in asthmatic patients receiving mechanical ventilation who have failed to respond to conventional ß-adrenergic agents (140). Experimental evidence indicates a direct effect on bronchial smooth muscle mediated via calcium-dependent channels, as well as by modulating vagal-, histamine-, allergen-, and hypoxia-induced bronchoconstrictor mechanisms (141,142). Furthermore, these agents reduce pulmonary vascular tone, resulting in lower pulmonary artery pressures in acute asthma (143). Bronchodilator responses are seen in the form of reduced peak airway pressures within minutes, associated with improved ventilation—resulting in a lower PaCO2—and reduced air trapping (144). Although the bronchodilator effects are seen at subanesthetic concentrations, these agents also offer a relatively expensive method of sedation. A few ICU ventilators, such as the Seimens Servo 900 series, can be fitted with a vaporizer, allowing anesthetic gases to be administered. Effective exhaled gas scavenging systems are required when using inhalational anesthetics in the ICU. If this system is not available, a Cardiff canister can be added to the expiratory port of the ventilator to remove effluent anesthetic gases. Significant side effects such as hypotension and myocardial irritability exist, and prolonged administration of some agents may result in bromide or fluoride toxicity (145). Sevoflurane, a halogenated ether, is largely devoid of cardiorespiratory side effects, and may be the preferred agent. The administration of subanesthetic concentrations of these agents via a face mask may relieve bronchospasm refractory to conventional treatment (146).
One of the difficult aspects of mechanical ventilation of the acute asthmatic patient is the weaning and extubation process. The presence of the endotracheal tube within the larynx and trachea induces bronchoconstriction, which becomes troublesome as the sedation is withdrawn in preparation for extubation (147,148). Use of an inhalational anesthetic agent allows the endotracheal tube to be removed under anesthesia, with the confident expectation of rapid recovery once the anesthetic is discontinued (149).
Special Procedures
Bedside Procedures and Monitoring
The long list of bedside ICU procedures includes special monitoring of critically ill patients, and provides guidance on all aspects of treatment, from the emergency room to the ICU. On that list, most are the commonly performed procedures used by critical care specialists, surgeons, emergency room physicians, and certified registered nurse anesthetists (Table 40.18) (150).
Mini-surgery
Bedside Diagnostic Minilaparoscopy and Minilaparotomy
The use of bedside minilaparoscopy as a diagnostic aid in the ICU patient with a possible intra-abdominal process is a rescue operation in a potential catastrophic condition. Although the workup of potential abdominal pathology in critically ill ICU patients uses conventional methods, including physical examination, CT, ultrasonography, and diagnostic peritoneal lavage, a delay in the diagnosis of intra-abdominal pathology is a major contributor to morbidity and mortality. The reasons for delay are multifactorial, including failure to consider the diagnosis, lack of sensitivity of noninvasive diagnostic modalities, and difficulty in safely transporting a critically ill patient. Bedside diagnostic laparoscopy is a modality that is safe, accurate, time efficient, and potentially therapeutic.
Recent laparotomy is no longer a contraindication to bedside laparoscopy. A recent study by Bauer et al. described the use of laparoscopy in patients with acute abdominal findings after urologic surgery (151). It is in the group of patients with recent previous laparotomy that diagnostic laparoscopy may have its greatest advantage over CT scanning. Postoperative changes may be difficult to differentiate from acute abdominal pathology on CT (e.g., free air, fluid, inflammation). Diagnostic laparoscopy, though, allows direct examination of the abdominal cavity. By avoiding negative laparotomies and limiting the reopening of recent abdominal incisions, it is possible to decrease wound complications and ultimately reduce the length of the hospital stay. Although not a new revelation, it is of significance to note that intubation is not a requirement for laparoscopy. Fabian et al. (152) showed that laparoscopy can be used safely in trauma patients. Diagnostic laparoscopy is often used as an operating room procedure under general anesthesia (152). Iberti et al. found it useful for identifying intestinal ischemia following aortobifemoral bypass (153). Others have described it as a tool that can be used outside the operating room, but exclusively to evaluate trauma by both blunt (154) and penetrating (155) mechanisms. Still others describe the use of diagnostic laparoscopy in the ICU; however, in this setting, the patient is required to be intubated and under general anesthesia (156,157); patients who have had a recent laparotomy are specifically excluded (157). The diagnosis of acute abdominal conditions in the critically ill patient remains difficult. ICU patients with abdominal pain, unexplained acidosis or sepsis, or suspected mesenteric ischemia are eligible for bedside diagnostic minilaparoscopy (158). Bedside minilaparoscopy can be a safe and accurate method to evaluate critically ill patients in whom the possibility of mesenteric ischemia or other intra-abdominal process is entertained. Bedside diagnostic laparoscopy can be a useful replacement for diagnostic laparotomy in the operating room. It should be included in the diagnostic algorithm when evaluating the unstable ICU patient with a suspected acute intra-abdominal process.
|
Table 40.18 List of all aspects of PROCEDURES AND MONITORING in the intensive care unit for which sedation or anesthesia is provided |
||
|
The procedure can be performed at the bedside in the ICU with the patient under local anesthesia and intravenous (conscious or asleep) sedation. In some reports (158,159) most of the patients did not require general anesthesia, although local anesthetics and sedation with midazolam or propofol were used. Most of the patients in these studies were intubated prior to laparoscopy. They required mechanical ventilation because of their disease process; none of them was intubated solely to perform the procedure. Local anesthesia with lidocaine and sedation with midazolam or propofol was used in all cases.
Pneumoperitoneum can be established with nitrous oxide (NO) to a relatively low pressure of 8 to 10 mm Hg.
Hemodynamics and ventilatory parameters should be monitored before, during, and after the procedure. Such procedures typically last a relatively short time (mean 21 minutes [158]). Laparoscopy performed at the bedside in the ICU may be used as a routine diagnostic tool in the evaluation of critically ill patients, similar to the use of CT, ultrasonography, and radiography (159), as there are minimal complications directly related to the procedure. Thus, bedside laparoscopy in the ICU under local or general anesthesia is a diagnostic and potentially therapeutic tool that can be used safely in the workup of potential abdominal pathology in critically ill patients. The application of diagnostic laparoscopy could become a routine procedure in the ICU to evaluate critically ill patients. No limitations, such as need for intubation or general anesthesia, should compromise the performance of the procedure. Additionally, patients with recent abdominal surgery were not excluded from consideration (159).
Laparoscopic Procedures
Laparoscopic procedures can reveal findings such as turbid fluid consistent with viscus perforation, sterile hemorrhagic fluid, a retroperitoneal mass, and an abdominal abscess (160). Thus, bedside laparoscopy in the ICU is feasible, informative, and accurate. It has a role in diagnosing abdominal pathologies and planning further treatment. It may avert a nontherapeutic laparotomy. Unfortunately, the prognosis in these patients is poor. Earlier use of this diagnostic modality may improve patient outcome.
Tracheostomy
Tracheostomy is one of the most frequent procedures carried out in critically ill patients, with major advantages compared to translaryngeal endotracheal intubation such as reduced laryngeal anatomic alterations, reduced inspiratory load, better patient tolerance, and improved nursing care. Thus, tracheostomy can enhance care in patients who need prolonged mechanical ventilation and/or airway control. The right timing for a tracheostomy remains controversial; however, it appears that early tracheostomy in selected severe trauma, burn, and neurologic patients could be effective to reduce the duration of mechanical ventilation, intensive care stay, and costs. ICU growth and improvements in technology have led to an increasing number of critically ill patients who require prolonged mechanical ventilation; these can be managed most appropriately with tracheostomies (161). Until recently, surgical tracheostomy performed in the OR was the only option available. However, morbidity from surgical tracheostomy ranges from 6% to 66%, and mortality ranges from 0% to 5% (162,163). Complications resulting from surgical tracheostomy performed in the ICU are comparable to those performed in the OR (162,163). The “classical” technique of percutaneous dilatational tracheostomy using progressive dilators was introduced by Ciaglia et al. in 1985 and, today, has become the procedure of choice in the majority of the cases, as it is safe, easy, and quick, with minor complications (164).
Percutaneous dilatational tracheostomy (PDT) has been recognized as a reliable alternative to the surgical placement of an artificial airway in patients with persistent respiratory failure due to various medical conditions (164,165). PDT may offer several advantages over conventional surgical tracheostomy placement, as PDT is associated with lower periprocedural and postprocedural complication rates (163); moreover, PDT can be performed at the bedside, thus avoiding the scheduling, time commitments, and costs associated with surgical operating facilities (Table 40.19A).
|
Table 40.19A Advantages of tracheostomy compared with oro-/nasotracheal intubation |
|
|
All PDT procedures are performed at the ICU bedside with continuous monitoring of blood pressure, heart rate, respiratory rate, oxygen saturation, and cardiac rhythm. Mechanical ventilatory support should be maintained throughout the procedure, the fraction of inspired oxygen increased to 1.0, and all patients placed on mandatory mechanical ventilation mode. Most procedures are attended by an anesthesiologist to assist in the management of the airway in the event of complications.
PDT has gained widespread acceptance in the ICU setting and presents a valid alternative to operative tracheostomy. In fact, recent data suggest several potential advantages compared to surgical tracheostomy, including ease of performance and a lower incidence of both peristomal bleeding and postoperative infection (166).
Among the relative contraindications for PDT are patients with altered neck anatomy due to severe neck burns and scarring from a previous tracheostomy (167). In addition, obese patients with large and thick necks are considered poor candidates for PDT, and are commonly referred for surgical tracheostomy placement (Table 40.19B).
Thrombocytopenia is another relative contraindication, and a higher incidence of bleeding, a prolonged stay in the ICU, and increased mortality are often associated with this finding (168). Many physicians consider thrombocytopenia a contraindication for performing the procedure (169,170); hence, thrombocytopenic patients often are excluded from comparative trials (166,171,172). PDT procedures take place under bronchoscopic control and are either performed or supervised by at least one pulmonologist or critical care medicine physician. Informed consent for these procedures is obtained from an appropriately designated surrogate. The procedure is performed in all patients following a standardized protocol, as previously described by Cantais et al. (171) using a commercially available kit (SIMS; Portex; Hythe, Kent, United Kingdom). The only modification consisted of the local administration of a 2% solution of lidocaine with epinephrine (1:200,000) before proceeding with tracheal puncture.
|
Table 40.19B Absolute and relative contraindications for percutaneous dilatational tracheostomy |
|
|
Immediately after the tracheostomy insertion, a bronchoscopic examination is performed through the tracheostomy to confirm the correct position of the tracheostomy tube and to identify injuries or bleeding. Subsequently, the trachea proximal to the percutaneously placed tracheostomy is inspected bronchoscopically via the remaining orotracheal tube to identify fractures of tracheal rings or blood. After the procedure, a chest radiograph was performed to rule out the presence of a pneumothorax.
Percutaneous Endoscopic Gastrostomy
Aspiration pneumonia due to gastroesophageal reflux is a frequent complication in ICU. The most commonly chosen method for long-term enteral access—gastrostomy—also reduces the risk of aspiration and shortens the hospital stay. A decrease in positive tracheal aspirate cultures was seen after PEG insertion—3.14 ± 1.95 times before PEG and 1.52 ± 1.47 times after PEG (173). Nasogastric tubes, used in the past, have been inadequate for long-term therapy due to patient discomfort, among other risks (174). The advantages of enteral versus parenteral feeding, in patients with a normal functioning gastrointestinal tract, are well known and include better patient compliance, maintenance of gastrointestinal tube integrity, and decreased costs, as well as minimizing villous atrophy and, at least theoretically, minimizing translocation of bacteria/fungi (174,175,176).
PEG placement seems to be a safe and cost-effective alternative to operative gastrostomy, especially as the latter requires general anesthesia and it is not without significant morbidity and mortality. Additionally, a failed PEG does not preclude subsequent operative gastrostomy. Surgical gastrostomy and jejunostomy are always performed in the operating theater with general anesthesia, and are associated with measurable morbidity and mortality (177). Ferraro et al. (178) performed PEG at the bedside in the ICU, using TIVA for patients with spontaneous ventilation and local anesthesia for sedated patients on mechanical ventilation. Enteral feeding through PEG usually started 24 hours after the end of the procedure. Early PEG in critically injured patients is a safe and effective method of providing access to the gastrointestinal tract for nutritional support. In patients with significant brain injuries, adequate sedation and the presence of an ICP monitor help to minimize secondary insults to the brain (179).
The indications for PEG placement are as follows: neurologic diseases with swallowing incapacity, pharyngeal and esophageal neoplasms, and long-term hospitalized patients after major surgical procedures who are unable to swallow. Absolute PEG contraindications are massive ascites, gastric varices, hepatomegaly, coagulopathy, and total esophageal stenosis. Previous abdominal surgery may not represent a problem if there is good adhesion between the abdominal and the gastric wall.
Burns and Wound Debridement
The main aim of care in a burn center is to control hypovolemia and obtain maximal tissue perfusion and oxygen delivery to damaged but viable tissues, as well as to healthy organs. To manage the burn shock, catecholamines are often indicated when appropriate fluid loading is inadequate to maintain perfusion. Mechanical ventilation is indicated in several cases: A deep burn over more than 60% of TBSA, facial and cervical burns, severe pulmonary burn injury from smoke inhalation, carbon monoxide intoxication, tracheobronchial thermal injury, and blast injury, among other reasons. Because of the severity of burn-related pain, continuous sedation is usually required. Early surgical treatment such as escharotomies, excision and grafting—which cause significant pain as well as blood loss—and hydrotherapy often require general anesthesia (180,181). Burn injury can modify the volume of distribution and the pharmacokinetics of anesthetic agents and muscle relaxants (181). Finally, chemical or electrical burns, radiation, associated CO intoxication, multiple trauma, and burn injury in infants raise specific problems.
The care of critically ill burn patients can be challenging because of the rapidly escalating tolerance for opioids. A recent study evaluated the safety and efficacy of anesthesiologist-administered anesthesia in the burn intensive care unit treatment room. The review suggested that these procedures can be performed safely with appropriate supervision and monitoring without detrimental effects on patient activity level or nutritional status (180).
Adequate analgesia is crucial in the critical care of burn victims. The quality and intensity of pain in severely burned patients during the ICU treatment changes frequently due to repeated operations and dressing changes. The administration of too much or too little analgesia can worsen outcome: Pain prolongs wound healing and immunologic incompetence, while overdosage of analgesics decreases intestinal motility and increases the length of stay at the ICU.
Greher et al. reported their first experiences with a new concept of analgesia—NSAIDs and narcotics—in severely burned ICU patients. This concept allowed adequate individual analgesia according to the actual demand without serious side effects. Analysis showed a reduction in cost by one third compared to a conventional analgesic regimen with sufentanil. This manner of analgesia provision in severely burned patients is safe, highly effective, and flexible enough to meet the actual analgesic demands of the patient. It can be used in both intubated and spontaneously breathing, nonintubated patients (134).
Ketamine is traditionally used for short- and long-term sedation and analgesia of a burn patient (181). Edrich et al. used ketamine for long-term sedation and analgesia of burn patients. Under escalating opiate dosages—even without adequate analgesia—the patient had developed persistent ileus as well as abdominal distension that caused respiratory compromise. The opiate-sparing effect of the continuous ketamine infusion allowed a decrement in dosage of more than 90%; the ileus resolved within 24 hours. The quality of sedation also changed for the better. There were no obvious adverse effects of ketamine (182).
Disease Treatment (Asthma, Epilepsy)
Status Epilepticus
Refractory status epilepticus (SE) is a major neurologic emergency, each year affecting 10 to 50 per 100,000 persons; in adults, its mortality rate ranges from 7% to 20% (183,184). Prompt initiation of treatment is essential, because SE becomes more refractory to treatment with time (183,184,185). SE that fails to respond to first-line therapy of benzodiazepines followed by second-line therapy (phenytoin, valproate, or phenobarbital) is defined as refractory SE (183,185). Refractory SE occurs in about 30% of patients with SE and is associated with a mortality rate of greater than 20% (183).
Management of refractory SE requires induction of coma with potent anesthetics under continuous EEG monitoring, requiring mechanical ventilation in an ICU setting. The aim of treatment is to terminate SE and prevent late SE-associated complications, including hyperthermia, hypotension, hypoglycemia, rhabdomyolysis, pulmonary edema, cerebral edema, and failure of cerebral autoregulation (185). Barbiturates are the anesthetics most commonly used to induce coma in this setting, especially in Europe (186,187). Propofol, the widely used intravenous anesthetic, has been shown to control SE in animals (188) and humans (189,190,191,192,193,194), and to shorten the duration of electroconvulsive therapy (195). It is still debated whether propofol should be used as an alternative to barbiturates or as first-choice treatment in refractory SE (196). A recent study showed that propofol was effective in the management of most refractory SE episodes in adults (196). Despite relatively high total doses of propofol, the incidence of treatment-related adverse events was quite low. In particular, no patient experienced life-threatening adverse effects or the so-called propofol infusion syndrome. The deaths were attributable to refractory SE itself or its etiology.
Propofol works possibly through modulation of GABA-α receptors at a site different from that targeted by benzodiazepines and barbiturates (188). Although propofol is currently considered as an alternative to barbiturates or midazolam for the management of patients with refractory SE (185), only limited clinical data are available. In a retrospective review of patients receiving propofol for refractory SE, it was found to be ineffective in only 14% (190). Another refractory SE series found no difference in terms of duration of ICU stay or the incidence of arterial hypotension between patients receiving propofol and those receiving barbiturates, whereas time to seizure control was significantly shorter in the propofol group (2.6 vs. 123 minute) (191). A retrospective comparison of propofol and midazolam in refractory SE did not find any difference in terms of seizure control (clinical or EEG), infectious complications, hemodynamic compromise, duration of mechanical ventilation, and mortality (193), and a recently published systematic review of 28 series—including 193 refractory SE patients (54 receiving midazolam, 33 propofol, and 106 barbiturates) (194)—showed that barbiturates were most effective for controlling seizures, followed by propofol and then midazolam; however, more patients receiving barbiturates had continuous EEG monitoring, introducing a possible bias. Furthermore, this study showed less hypotension with propofol, suggesting possible subtherapeutic dosage of propofol. Finally, propofol was recently reported to control complex-partial refractory SE (192). In the study of Rossetti et al. (196), 77% of refractory SE episodes were successfully treated, allowing permanent seizure control in 67% of patients with propofol alone, and 10% with propofol and subsequent barbiturate therapy. Propofol was administered at relatively high doses (mean, 4.8 mg/kg/hour) for several days (mean, 3 days). The overall mortality rate was 23%, which is identical to that found in another retrospective refractory SE study (183). The large variation in previously reported mortality rates, ranging from 17% to 80%, can be explained by discrepancies in the definition, management, and etiology of refractory SE (183,191,197,198). The median duration of mechanical ventilation and ICU stay in the Mayer study (183) were shorter than previously reported in series of refractory SE treated with barbiturates (197,198). However, discrepancies in patient selection between series may account for these differences. The relatively short duration of mechanical ventilation may be related to the pharmacokinetic properties of propofol, especially its short elimination half-life (190,191).
To our knowledge, no fatal case of propofol infusion syndrome has been described in patients with refractory SE. Although some of the patients had high propofol infusion rates for a prolonged time (i.e., ≥9 days), isolated hyperlipidemia was rarely seen (196).
Some patients with long propofol treatment had transient movement disorders, showing tremor on emergence from general anesthesia and transient focal dystonia of a limb. Whereas some case reports underlined the efficacy of propofol in the management of refractory SE (189), others described abnormal movements, posturing, and seizurelike activity related to its use (199,200). Other studies—prospectively investigating motor phenomena related to propofol by using EEG monitoring—concluded that these were nearly always nonepileptic (201). It is thus likely that the aforementioned “seizures” might have been confused with abnormal movements, including opisthotonus, increased tone with twitching, and rhythmic movements (202,203), which are probably caused by subcortical dopaminergic excitatory activity induced by a low dose of propofol. These movements disappear as cortical GABA inhibition occurs at higher doses (201). Propofol might also act as a glycine antagonist in subcortical and spinal structures (203), explaining the occurrence of opisthotonus. Similar abnormal movements can be encountered with many other anesthetics (204).
Status Asthmaticus
Status asthmaticus is defined as an attack of bronchial asthma that resists conventional treatment and continues for more than 24 hours. Most deaths from acute asthma occur outside the hospital, but the at-risk patient may be recognized on the basis of prior ICU admission and asthma medication history. Patients who fail to improve significantly in the emergency department should be admitted to an ICU for observation, monitoring, and treatment. Hypoxia, dehydration, acidosis, and hypokalemia render the severe acute asthmatic patient vulnerable to cardiac dysrhythmia and cardiorespiratory arrest. Mechanical ventilation may be required for a small proportion of patients for whom it may be life saving. Aggressive bronchodilator (e.g., continuous nebulized ß-agonist treatment) and anti-inflammatory therapy must continue throughout the period of mechanical ventilation. Recognized complications of mechanical ventilation include hypotension, barotrauma, and nosocomial pneumonia. Low ventilator respiratory rates, long expiratory times, and small tidal volumes help to prevent hyperinflation. Volatile anesthetic agents may produce bronchodilation in patients resistant to ß agonists. Fatalities in acute asthmatics admitted to the ICU are relatively uncommon (205).
Drug Therapy for Intubation and Mechanical Ventilation in Status Asthmaticus
Anesthetic Agents and Sedatives
Etomidate and thiopentone are short-acting imidazole and barbiturate drugs, respectively, that are commonly used for intubation, although there are rare reports of bronchospasm and anaphylactoid reactions with these agents. Longer-term sedation may be obtained by infusion of midazolam (2–10 mg/hour), although metabolites may accumulate in renal and hepatic impairment. Ketamine is a general anesthetic agent that has been used before, during, and after intubation in patients with acute severe asthma. It has sympathomimetic and bronchodilating properties. The usual dose for intubation is 1 to 2 mg/kg given intravenously over 2 to 4 minutes. It may increase blood pressure and heart rate, lower seizure threshold, alter mood, and cause delirium. Inhalational anesthetics used as induction agents have the advantage of bronchodilation and may make muscle relaxation unnecessary; however, specialized anesthetic equipment is required for this approach.
Opioids are a useful addition to sedatives and provide analgesia during intubation and mechanical ventilation. Morphine as a bolus may cause histamine release, which can worsen bronchoconstriction and hypotension. Some intravenous preparations also contain metabisulphite, to which some asthmatics are sensitive. Fentanyl is a better choice of opioid for intubation as it inhibits airway reflexes and is short acting. It causes less histamine release than morphine, but large boluses may cause bronchospasm and chest wall rigidity.
Neuromuscular Blocking Drugs
Rocuronium, a nondepolarizing muscle relaxant with an acceptably rapid onset, offers an alternative to succinylcholine. Allergic sensitivity may occur to any neuromuscular blocking agent, and many may also cause histamine release with the potential for bronchospasm, particularly in bolus doses. Atracurium boluses should be avoided because of the bronchospastic potential, and vecuronium or pancuronium infusions should be used for longer-term maintenance of muscle relaxation.
Myopathy and muscle weakness are well-recognized complications of the long-term administration of nondepolarizing neuromuscular blocking agents in asthmatic patients, with an incidence of about 30%. In most cases, the myopathy is reversible, but may take weeks to resolve. There is an association between neuromyopathy and the duration of muscle relaxant drug use that is independent of corticosteroid therapy. The use of neuromuscular blocking agents should, therefore, as possible be kept to a minimum.
Inhalational Anesthetic Agents: The Nonresponding Patient
Status asthmaticus can be successfully treated with volatile anesthetics such as isoflurane. The tidal volume, pH, and PaCO2 can be improved within 6 hours after anesthesia (205). When patients who were not treated with isoflurane were compared to patients treated with the agent in an attempt to assess the usefulness of isoflurane inhalation therapy, isoflurane inhalation therapy seemed useful for intractable status asthmaticus, and earlier introduction of this agent was expected to achieve a greater therapeutic effect (205). The patients treated with isoflurane stayed in the ICU and underwent mechanical ventilation for a shorter period. These patients had hypotension and liver dysfunctionafter the inhalation anesthesia, but these symptoms were improved by decreasing the concentration of isoflurane.
Halothane, isoflurane, and sevoflurane are potent bronchodilators in asthmatic patients receiving mechanical ventilation who have failed to respond to conventional ß-adrenergic agents. Experimental evidence indicates a direct effect on bronchial smooth muscle mediated via calcium-dependent channels as well as by modulating vagal-, histamine-, allergen-, and hypoxia-induced bronchoconstrictor mechanisms. Furthermore, these agents reduce pulmonary vascular tone, resulting in lower pulmonary artery pressures in acute asthmatic episodes. Bronchodilator responses are seen in the form of reduced peak airway pressures within minutes, associated with improved distribution of ventilation—resulting in a lower PaCO2—and reduced air trapping. Although bronchodilator effects are seen at subanesthetic concentrations, these agents also offer a relatively expensive method of sedation. Several ICU ventilators, such as the Seimens Servo 900 series, can be fitted with a vaporizer, which allows anesthetic gases to be administered. Effective exhaled gas scavenging systems are required when using inhalational anesthetics in the ICU. Significant side effects such as hypotension and myocardial irritability exist, and prolonged administration of some agents may result in bromide or fluoride toxicity. The halogenated ether sevoflurane is largely devoid of cardiorespiratory side effects and may be the preferred agent. Administration of subanesthetic concentrations of one of these agents via face mask may relieve bronchospasm refractory to conventional treatment.
Imaging and Interventional Radiology
Among the long list of bedside procedures in the ICU that require special monitoring and care of the critically ill patient are MRI and CT scan, umbrella insertion, and angiographic manipulation (150). Among the critically ill, there is a significant incidence of death after diagnostic procedures (Fig. 40.8) (13), probably related to the aggressive use of diagnostic techniques (CT, MRI) in seriously ill patients, which mandates the use of general anesthesia or anesthesia care and monitoring during transport and the procedure.
Umbrella Insertion or Inferior Vena Cava Filter
For some ICU patients—at high risk for development of deep vein thrombosis and pulmonary embolism but with contraindications for anticoagulation therapy—the inferior vena cava filters are very useful and safe. Inferior vena cava filters are traditionally placed in the angio suite or operating room under fluoroscopy. Performing the procedure under such circumstances, in spite of being very efficient, presents two inconveniences: The need to transport the patient to the site where the fluoroscopy equipment is located and the use of iodinated contrast for proper location, and release of the devices. For patients with normal renal function and for those with conditions that require them being taken to the procedure room, such facts do not seem relevant. However, for patients with compromised renal function—mainly those on the edge of acute kidney failure—the use of iodinated contrast, even in small quantities, may cause worsening of the nephrologic prognosis. On the other hand, critically ill patients who are hemodynamically unstable, are dependent on mechanical ventilation, and require high fractions of O2 often present a high risk and are not candidates for transportation to environments with fluoroscopy to insert inferior vena cava filters. There are reports indicating an increased risk for complications—from 5.9% to 15.5%—during the intrahospital transportation of critically ill patients (206,207,208). For patients in these circumstances, it may be more appropriate to perform bedside procedures if possible. Some authors described the use of ultrasound for inferior vena cava filter placement, with a 97% success rate (209). Moreover, the vena cava filter placement guided by ultrasound seems to be effective, safe, and economically advantageous in relation to the conventional method (210,211).
|
|
|
Figure 40.8. The rate of mortality by type of surgery for patients in the American Society of Anesthesiologists Physical Status (ASA PS) V category. Mortality rate was the highest in the abdominal surgery and the diagnostic procedures groups. (From Sidi A, Lobato EB, Cohen JA. The American Society of Anesthesiologists Physical Status: category V revisited. J Clin Anesth. 2000;12:328–334.) |
Summary
Most ICU patients require analgesia and sedation for pain and anxiety management and mechanical ventilation, or as adjuvant therapy for bedside procedures done in the ICU. These patients may undergo surgical interventions outside the traditional OR procedures. The roots of CCM are to be found in anesthesiology, extending the OR care delivered to the critically ill to the PACU. The needs of these high-acuity patients led to the development of better OR monitoring and more aggressive management. In that regard, anesthesiology and intensive care medicine influenced and fertilized one another, and this symbiosis was mostly positive. Of course, problems may occur with long-term ICU use of drugs initially conceived for short-term OR anesthetic use. It is not just drugs from the OR, but also monitoring devices that are of interest to intensivists, such as the pulmonary artery catheter and the BIS monitor.
Perioperative mortality is a product of the severity of illness, the advances in life support, and our interventions that affect the rate of acute mortality. To determine our priorities while practicing anesthesia in the ICU environment, we need to learn and assess patient risk and safety in the ICU.
Sedation is an essential component in the management of intensive care patients. It is required to relieve the discomfort and anxiety caused by procedures such as tracheal intubation, ventilation, suction, and physiotherapy. It can also minimize agitation and maximize rest and appropriate sleep. Analgesia is an almost universal requirement for the intensive care patient. Adequate sedation and analgesia ameliorates the metabolic response to surgery and trauma. Too much or too little sedation and analgesia can increase morbidity. Sedative/analgesic dosage of commonly used agents varies between patients. A valid method for monitoring sedation would allow sedation to be tailored to the individual. Any scoring system should be simple, easily performed, noninvasive, and, most importantly, reproducible. Physiologic variables, serum concentrations of drugs, and neurophysiologic tools such as EEG have all been used but proven to be expensive and unreliable. The challenge for critical care physicians who use analgesics and sedatives is to provide patient comfort and safety without increasing morbidity and mortality. Because of the variety in practice styles, pathways to standardize patient care have attracted attention. From a mechanical ventilation standpoint, weaning protocols have been shown to improve efficiency, reduce resource utilization, improve patient outcomes, reduce overall ICU expenditures, and decrease the frequency of tracheostomies.
ICU sedation poses many problems. The action and side effects of intravenous drugs in the severely ill patient population of an ICU are difficult to control. The incidence of posttraumatic stress disorder after long-term sedation is high. The recent focus on propofol infusion syndrome entails restrictions in the use of this drug. On the other hand, volatile anesthetics very selectively suppress consciousness but leave many autonomic functions intact. In the absence of perception, processing the number of adverse experiences should be lower, leading to a better psychological outcome. Respiration and intestinal motility are not depressed, facilitating modern therapeutic modalities such as early enteral feeding and augmentation of spontaneous breathing. Awakening after inhalational ICU sedation is quick and predictable; extubation can be planned and organized, and the time during which the patient needs very close observation will be short.
ICU management of critically ill patients often includes anesthesia for minor procedures such as tracheostomy and percutaneous endoscopic gastrostomy tube. Prospective planning requires knowledge of the patient's condition and an assessment of the anesthetic requirements of the proposed procedure. The spectrum of anesthetic options ranges from sedation and analgesia and monitored anesthesia care, tototal intravenous anesthesia.
References
1. Maccioli GA, Cohen NH. General anesthesia in the intensive care unit? Is it ready for “prime time”? Criti Care Med. 2005;33(3):687–688.
2. Lassen HCA. A preliminary report on the 1952 epidemic of poliomyelitis in Copenhagen with special reference to the treatment of acute respiratory insufficiency. Lancet. 1953;1:37–40.
3. Bjork VO, Engstrom CG. The treatment of ventilatory insufficiency after pulmonary resection by tracheostomy and artificial ventilation. J Thorac Surg. 1957;34:228–241.
4. Ramsay JG. Anesthesiology in critical care medicine: a symbiosis? ASA Newslett. 2000;64(3).
5. Lassen HCA, Hinriksen E, Neukirch F, et al. Treatment of tetanus: Severe bone marrow suppression after prolonged nitrous oxide anesthesia. Lancet. 1956;1:527–530.
6. Ledingham IM, Finlay WEI, Watt I, et al. Etomidate and adrenocortical function (letter). Lancet. 1983;1:1434.
7. Watling SM, Dasta JF. Prolonged paralysis in intensive care unit patients after the use of neuromuscular blocking agents: a review of the literature. Crit Care Med. 1994;22:884–893.
8. Cray SH, Robinson BH, Cox PN. Lactic acidemia and bradyarrhythmia in a child sedated with propofol. Crit Care Med. 1998;26:2087–2092.
9. Kang TM. Propofol infusion syndrome in critically ill patients. Ann Pharmacother. 2002;36:1453–1456.
10. Connors AF, Speroff T, Dawson NV, et al. The effectiveness of right heart catheterization in the initial care of critically ill patients. JAMA. 1996;276:889–897.
11. De Deyne C, Struys M, Decruyenaere J, et al. Use of continuous bispectral EEG monitoring to assess depth of sedation in ICU patients. Intens Care Med. 1998;24:1294–1298.
12. Ashbaugh DG, Bigelow DB, Petty TL, et al. Acute respiratory distress syndrome in adults. Lancet. 1967;2:319–323.
13. Sidi A, Lobato EB, Cohen JA. The American Society of Anesthesiologists Physical Status: category V revisited. J Clin Anesth. 2000;12:328– 334.
14. Trunkey DD. Trauma. Sci Am. 1983;249:28.
15. Keats AS. The ASA classification of physical status—a recapitulation. Anesthesiology. 1978;49:233–236.
16. Saklad M. Grading of patients for surgical procedures. Anesthesiology. 1941;2:281–284.
17. New Classification of Physical Status. American Society of Anesthesiologists, Inc. Anesthesiology. 1963;24:111.
18. Dripps RD, Lamont A, Eckenhoff JE. The role of anesthesia in surgical mortality. JAMA. 1961;178:261–266.
19. Preoperative evaluation and the choice of anesthetic techniques. In: Stoelting RK, Miller RD, eds. Basics of Anesthesia. 3rd ed. New York: Churchill Livingstone; 1994:108.
20. Vacanti CJ, vanHouten RJ, Hill RC. A statistical analysis of the relationship of physical status to postoperative mortality in 68,388 cases. Anesth Analg. 1970;49:564–566.
21. Marx GF, Mateo CV, Orkin LR. Computer analysis of postanesthetic deaths. Anesthesiology. 1973;39:54–58.
22. Keats AS. The ASA classification of physical status—a recapitulation. Anesthesiology. 1978;49:233–236.
23. Owens WD, Felts JA, Spitznagel EL. ASA physical status classifications. Anesthesiology. 1978;49:239–243.
24. Warden JC, Horan BF. Deaths attributed to anaesthesia in New South Wales, 1984–1990. Anaesth Intensive Care. 1996;24:66–73.
25. Cullen DJ, Nemeskal AR, Cooper JB, et al. Effect of pulse oximetry, age, and ASA physical status on the frequency of patients admitted unexpectedly to a postoperative intensive care unit and the severity of their anesthesia-related complications. Anesth Analg. 1992;74:181–188.
26. Ruiz K, Aitkenhead AR. Was CEPOD right? Anaesthesia. 1990;45:978–980.
27. Forrest JB, Rehder K, Cahalan MK, et al. Multicenter study of general anesthesia. III. Predictors of severe perioperative adverse outcomes. Anesthesiology. 1992;76:3–15.
28. Tiret L, Hatton F, Desmonts JM, et al. Prediction of outcome of anaesthesia in patients over 40 years: a multifactorial risk index. Stat Med. 1988;7:947–954.
29. Leardi S, De Santis C, Ciccarelli O, et al. Risk of surgery in the geriatric age: prospective evaluation of risk factors. Ann Ital Chir. 1998;69:575–579.
30. Leardi S, De Santis C, Ciuca B, et al. Risk indices in geriatric surgery: ASA index versus Reiss index. Minerva Chir. 1997;52:255–260.
31. Wahl W, Pelletier K, Schmidtmann S, et al. Experience with various scores in evaluating the prognosis of postoperative intensive care patients. Chirurg. 1996;67:710–717.
32. Wolters U, Wolf T, Stutzer H, et al. ASA classification and perioperative variables as predictors of postoperative outcome. Br J Anaesth. 1996;77:217–222.
33. Hall JC, Hall JL. ASA status and age predict adverse events after abdominal surgery. J Qual Clin Pract. 1996;16:103–108.
34. Hessman O, Bergkvist L, Strom S. Colorectal cancer in patients over 75 years of age—determinants of outcome. Eur J Surg Oncol. 1997;23:13–19.
35. Goffi L, Saba V, Ghiselli R, et al. Perioperative APACHE II and ASA scores in patients having major general surgical operations: prognostic value and potential clinical applications. Eur J Surg. 1999;165:730–735.
36. Di Paolo S, Giangreco L, Staudacher C. Operative risk in elderly patients with gastrointestinal hemorrhage. Minerva Chir. 1996;51:953–957.
37. Groenendijk RP, Croiset van Uchelen FA, Mol SJ, et al. Factors related to outcome after pneumonectomy: retrospective study of 62 patients. Eur J Surg. 1999;165:193–197.
38. Goldstein A Jr, Keats AS. The risk of anesthesia. Anesthesiology. 1970;33:130–143.
39. Waters J, Wilkinson C, Golmon M, et al. Evaluation of cardiac risk in noncardiac surgical patients [Abstract]. Anesthesiology. 1981;55:A343.
40. Schwilk B, Muche R, Bothner U, et al. Quality control in anesthesiology. Results of a prospective study following the recommendations of the German Society of Anesthesiology and Intensive Care. Anaesthetist. 1995;44:242–249.
41. Del Guercio LRM, Cohn JD. Monitoring operative risk in the elderly. JAMA. 1980;243:1350–1355.
42. Anon. New classification of physical status. Anesthesiology. 1963;24:111.
43. Buck N, Devlin HB, Lunn JN. The Report of a Confidential Enquiry into Perioperative Deaths. London: The Nuffield Provincial Hospitals Trust and Kings Fund; 1987.
44. Bein R, Fröhlich D, Pömsl J, et al. The predictive value of four scoring systems in liver transplant recipients. Intens Care Med. 1995;21:32–37.
45. Turner JS, Morgan CJ, Thakrar B, et al. Difficulties in predicting outcome in cardiac surgery patients. Crit Care Med. 1995;23:1843–1850.
46. Le Gall J-R, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA. 1993;270:2957–2963.
47. Parsonnet V, Dean D, Bernstein AD. A method of uniform stratification of risk for evaluating the results of surgery in acquired adult heart disease. Circulation. 1989;79(suppl I):3–12.
48. Goldman L, Caldera DL, Nussbaum SR, et al. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med. 1977;297(16):845–850.
49. Ross AF, Tinker JH. Cardiovascular disease. In: Brown DL, ed. Risk and Outcome in Anesthesia. Philadelphia: JB Lippincott Co; 1988:39.
50. Schoeppel SL, Wilkinson C, Waters J, et al. Effects of myocardial infarction on perioperative cardiac complications. Anesth Analg. 1983;62(5):493–498.
51. Jeffrey CC, Kunsman J, Cullen DJ, et al. A prospective evaluation of cardiac risk index. Anesthesiology. 1983;58(5):462–464.
52. Detsky AS, Abrams HB, McLaughlin JR, et al. Predicting cardiac complications in patients undergoing non-cardiac surgery. J Gen Intern Med. 1986;1(4):211–219.
53. Detsky AS, Abrams HB, Forbath N, et al. Cardiac assessment for patients undergoing noncardiac surgery. A multifactorial clinical risk index. Arch Intern Med. 1986;146(11):2131–2134.
54. Dupuis JY, Wang F, Nathan H, et al. The cardiac anesthesia risk evaluation score: a clinically useful predictor of mortality and morbidity after cardiac surgery. Anesthesiology. 2001;94(2):194–204.
55. Tuman KJ, McCarthy RJ, March RJ, et al. Morbidity and duration of ICU stay after cardiac surgery. A model for preoperative risk assessment. Chest. 1992;102:36–44.
56. Tu JV, Jaglal SB, Naylor D, the Steering Committee of the Provincial Adult Care Network of Ontario. Multicenter validation of a risk index for mortality, intensive care unit stay, and overall hospital length of stay after cardiac surgery. Circulation. 1995;91:677–684.
57. Peter K, Lutz H. [Proceedings: Preoperative exploration (author's trans.)]. Langenbecks Arch Chir. 1973;334:681–687.
58. Goldman L. Perioperative myocardial ischemia. To everything there is a season. Anesthesiology. 1992;76(3):331–333.
59. Goldman L. Cardiac risk in noncardiac surgery: an update [Review]. Anesth Analg. 1995;80(4):810–820.
60. Foster ED, Davis KB, Carpenter JA, et al. Risk of noncardiac operation in patients with defined coronary disease: the Coronary Artery Surgery Study (CASS) registry experience. Ann Thorac Surg. 1986;41(1):42–50.
61. Knudsen NW, Sebastian MW, Perez-Tamayo RA, et al. Intensive care unit procedures: cost savings and patient safety. Crit Care. 1999;3(suppl 1):P2.
62. Lewis KS, Whipple JK, Michael KA, et al. Effect of analgesic treatment on the physiological consequences of acute pain. Am J Hosp Pharm. 1994;51(12):1539–1554.
63. Mangano DT, Siliciano D, Hollenberg M, et al. Postoperative myocardial ischemia. Therapeutic trials using intensive analgesia following surgery. The Study of Perioperative Ischemia (SPI) Research Group. Anesthesiology. 1992;76(3):342–353.
64. Britton BJ, Hawkey C, Wood WG, et al. Stress—a significant factor in venous thrombosis? Br J Surg. 1974;61(10):814–820.
65. Slade MS, Greenberg LJ, Yunis EJ, et al. Integrated immune response to standard major surgical trauma in normal patients. Surg Forum. 1974;25(0):425–427.
66. Swinamer DL, Phang PT, Jones RL, et al. Effect of routine administration of analgesia on energy expenditure in critically ill patients. Chest. 1988;93(1):4–10.
67. Moller IW, Dinesen K, Sondergard S, et al. Effect of patient-controlled analgesia on plasma catecholamine, cortisol and glucose concentrations after cholecystectomy. Br J Anaesth. 1988;61(2):160–164.
68. Modig J, Borg T, Bagge L, et al. Role of extradural and of general anaesthesia in fibrinolysis and coagulation after total hip replacement. Br J Anaesth. 1983;55(7):625–629.
69. Salomaki TE, Leppaluoto J, Laitinen JO, et al. Epidural versus intravenous fentanyl for reducing hormonal, metabolic, and physiologic responses after thoracotomy. Anesthesiology. 1993;79(4):672–679.
70. Jones C, Griffiths RD, Macmillan RR, et al. Psychological problems occurring after intensive care. Br J Int Care. 1994;2:46–53.
71. Parker MM, Schubert W, Shelhamer JH, et al. Perceptions of a critically ill patient experiencing therapeutic paralysis in an ICU. Crit Care Med. 1984;12(1):69–71.
72. Schelling G, Stoll C, Haller M, et al. Health-related quality of life and posttraumatic stress disorder in survivors of the acute respiratory distress syndrome. Crit Care Med. 1998;26(4):651–659.
73. Bond M. Psychological and psychiatric aspects of pain. Anaesthesia. 1978;33(4):355–361.
74. Chapman CR, Casey KL, Dubner R, et al. Pain measurement: an overview. Pain. 1985;22(1):1–31.
75. Ramsay MA, Savege TM, Simpson BR, et al. Controlled sedation with alphaxalone-alphadolone. BMJ. 1974;2(920):656–659.
76. Shapiro BA. Bispectral Index: better information for sedation in the intensive care unit? Crit Care Med. 1999;27(8):1663–1664.
77. Liu J, Singh H, White PF. Electroencephalographic bispectral index correlates with intraoperative recall and depth of propofol-induced sedation. Anesth Analg. 1997;84(1):185–189.
78. Shah N, Clack S, Chea F, et al. Does bispectral index of EEG correlate with Ramsay sedation score in ICU patients [Abstract]? Anesthesiology. 1996;85:A469.
79. Frenzel D, Greim CA, Sommer C, et al. Is the bispectral index appropriate for monitoring the sedation level of mechanically ventilated surgical ICU patients? Intensive Care Med. 2002;28(2):178–183.
80. De Deyne C, Struys M, Decruyenaere J, et al. Use of continuous bispectral EEG monitoring to assess depth of sedation in ICU patients. Intensive Care Med. 1998;24(12):1294–1298.
81. Jacobi J, Fraser GL, Coursin DB, et al. Task Force of the American College of Critical Care Medicine (ACCM) of the Society of Critical Care Medicine (SCCM), American Society of Health-System Pharmacists (ASHP), American College of Chest Physicians Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med. 2002;30(1):119–141.
82. Cohen AT, Kelly DR. Assessment of alfentanil by intravenous infusion as long term sedation in intensive care. Anaesthesia. 1987;42:545–548.
83. O'Sullivan G, Park GR. The assessment of sedation in critically ill patients. Clin Intensive Care. 1991;2:116–122.
84. Armstrong RF, Bullen C, Cohen SL, et al. Intermittent positive pressure ventilation. Clin Intensive Care. 1992;3:284–287.
85. Cook S. Technical Problems in Intensive Care. Intensive Care Rounds. Abingdon, UK: The Medicine Group Ltd.; 1991:19–22.
86. Schulte-Tamburen AM, Scheier J, Briegel J, et al. Comparison of five sedation scoring systems by means of auditory evoked potentials. Intensive Care Med. 1999;25:377–382.
87. Thornton C, Barrowcliffe MP, Konieczko KM, et al. The auditory evoked response as an indicator of awareness. Br J Anaesth. 1989;63:113–115.
88. Cohen IL. The management of the agitated ICU patient. Crit Care Med. 2002;30(Suppl. 1):S97–123.
89. Bell DM, Richards G, Dhillon S, et al. A comparative pharmacokinetic study of intravenous and intramuscular midazolam in patients with epilepsy. Epilepsy Res. 1991;10:183–190.
90. Shelly MP, Mendel L, Park GR. Failure of critically ill patients to metabolise midazolam. Anaesthesia. 1987;42:619–626.
91. Greenblatt DJ, Divoll MK, Soong MH, et al. Desmethyldiazepam pharmacokinetics: studies following intravenous and oral desmethyldiazepam, oral clorazepate, and intravenous diazepam. J Clin Pharmacol. 1988;28:853–859.
92. Barrientos-Vega R, Sanchez-Soria M, Morales-Garcia C, et al. Prolonged sedation of critically ill patients with midazolam or propofol: impact on weaning and costs. Crit Care Med. 1997;25:33–40.
93. Dirksen MS, Vree TB, Driessen JJ. Clinical pharmacokinetics of long-term infusion of midazolam in critically ill patients—preliminary results. Anaesth Intensive Care. 1987;15:440–444.
94. Shelly MP, Sultan MA, Bodenham A, et al. Midazolam infusions in critically ill patients. Eur J Anaesthesiol. 1991;8:21–27.
95. Finfer SR, O'Connor AM, Fisher MM. A prospective randomised pilot study of sedation regimens in a general ICU population: a reality-based medicine study. Crit Care. 1999;3(3):79–83.
96. Van Hamme MJ, Ghoneim MM, Ambre JJ. Pharmacokinetics of etomidate, a new intravenous anesthetic. Anesthesiology. 1978;49(4):274–277.
97. Wagner RL, White PF, Kan PB, et al. Inhibition of adrenal steroidogenesis by the anesthetic etomidate. N Engl J Med. 1984;310(22):1415–1421.
98. Shapiro BA, Warren J, Egol AB, et al. Practice parameters for intravenous analgesia and sedation for adult patients in the intensive care unit: An executive summary. Society of Critical Care Medicine. Crit Care Med. 1995;23:1596–1600.
99. Glass PSA, Hardman D, Kamiyama Y, et al. Preliminary pharmacokinetics and pharmacodynamics of an ultra-short-acting opioid: remifentanil (GI87084B). Anesth Analg. 1993;77:1031–1040.
100. Dahaba AA, Grabner T, Rehak P, et al. Remifentanil versus morphine analgesia and sedation for mechanically ventilated critically ill patients: a randomized double blind study. Anesthesiology. 2004;101(3):640–646.
101. Cavaliere F, Antonelli M, Arcangeli A, et al. A low-dose remifentanil infusion is well tolerated for sedation in mechanically ventilated, critically-ill patients. Can J Anesth. 2002;49:1088–1094.
102. Riker RR, Picard JT, Fraser GL. Prospective evaluation of the Sedation-Agitation Scale for adult critically ill patients. Crit Care Med. 1999;27:1325–1329.
103. Segal IS, Vickery RG, Walton JK, et al. Dexmedetomidine diminishes halothane anesthetic requirements in rats through postsynaptic alpha-2 adrenergic receptor. Anesthesiology. 1988;69:818–823.
104. Urwin1 SC, Menon DK. Review article: comparative tolerability of sedative agents in head-injured adults. Drug Saf. 2004;27(2):107–133.
105. Asgeirsson B, Grande PO, Nordstrom CH, et al. Effects of hypotensive treatment with β2-agonist and β1-agonist on cerebral haemodynamics in severely head injured patients. Acta Anaesthesiol Scand. 1995;39:347–351.
106. Soliman H, Melot C, Vincent J. Sedative and analgesic practice in the intensive care unit: the results of a European survey. Br J Anaesth. 2001;87(2):186–192.
107. Christensen BV, Thunedborg LP. Use of sedatives, analgesics and neuromuscular blocking agents in Danish ICUs 1996/97: a national survey. Intensive Care Med. 1999;25(2):186–191.
108. Murdoch S, Cohen A. Intensive care sedation: a review of current British practice. Intensive Care Med. 2000;26(7):922–928.
109. Liu LL, Gropper MA. Review: postoperative analgesia and sedation in the adult intensive care unit. A guide to drug selection. Drugs. 2003;63(8):755–767.
110. Ely EW, Baker AM, Dunagan DP, et al. Effect on the duration of mechanical ventilation of identifying patients capable of breathing spontaneously. N Engl J Med. 1996;335(25):1864–1869.
111. Brook AD, Ahrens TS, Schaiff R, et al. Effect of a nursing-implemented sedation protocol on the duration of mechanical ventilation. Crit Care Med. 1999;27(12):2609–2615.
112. Kress JP, Pohlman AS, O'Connor MF, et al. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342(20):1471–1477.
113. Proctor S. Is this the end of research as we know it? BMJ. 1997;315(7105): 388.
114. Jacobs JR, Reves JG, Glass PSA. Rationale and technique for continuous infusions in anesthesia. Int Anesthesiol Clin. 1991;29:23–38.
115. Shelly MP. Sedation, where are we now? Intensive Care Med. 1999;25:137–139.
116. Olsson GL, Leddo CC, Wild L. Nursing management of patients receiving epidural narcotics. Heart Lung. 1989;18:130–138.
117. Covington H. Use of propofol for sedation in the ICU. Crit Care Nurse. 1998;18(4):34–39.
118. Halpern NA, Bettes L, Greenstein R. Federal and nationwide intensive care units and healthcare costs: 1986–1992. Crit Care Med. 1994;22:2001–2007.
119. Gundlach CA, Faulkner TP, Souney PF. Drug usage patterns in the ICU: profile of a major metropolitan hospital and comparison with other ICUs. Hosp Formul. 1991;26:132–136.
120. Cheng EY. The cost of sedating and paralyzing the critically ill patient. Crit Care Clin. 1995;11:1005–1019.
121. 1999 New York Times Almanac. New York: Penguin Reference Books; 1998:316.
122. Kress JP, O'Connor MF, Pohlman AS, et al. Sedation of critically ill patients during mechanical ventilation: a comparison of propofol and midazolam. Am J Respir Crit Care Med. 1996;153:1012–1018.
123. Swart EL, van Schijndel RJM, van Loenen AC, et al. Continuous infusion of lorazepam versus midazolam in patients in the intensive care unit: sedation with lorazepam is easier to manage and is more cost-effective. Crit Care Med. 1999;27:1461–1465.
124. Sivam SP, Ho IK. GABA in morphine analgesia and tolerance. Life Sci. 1985;37:199–208.
125. Ronan KP, Gallagher TJ, George B, et al. Comparison of propofol and midazolam for sedation in intensive care unit patients. Crit Care Med. 1995;23:286–293.
126. Mirski MA, Muffelman B, Ulatowski JA, et al. Sedation for the critically ill neurologic patient. Crit Care Med. 1995;23:2038–2053.
127. Braman SS, Dunn SM, Amico CA, et al. Complications of intrahospital transport in critically ill patients. Ann Intern Med. 1987;107:469–473.
128. Indeck M, Peterson S, Smith J, et al. Risk, cost, and benefit of transporting ICU patients for special studies. J Trauma. 1988;28:1020–1025.
129. Shah S. ICU Analgesia/Sedation Guidelines Created. Current Topics from the Drug Information Center, College of Pharmacy, University of Kentucky; 2000;30(1):1–4.
130. Shafer SL. Advances in propofol pharmacokinetics and pharmacodynamics. J Clin Anesth. 5;(6 Suppl 1):15S.
131. Westmoreland CL, Hoke JF, Sebel PS, et al. Pharmacokinetics of remifentanil (GI87084B) and its major metabolite (GI90291) in patients undergoing elective inpatient surgery. Anesthesiology. 1993;79(5):893–903.
132. Matta B, Menon D. Severe head injury in the United Kingdom and Ireland: a survey of practice and implications for management. Crit Care Med. 1996;24:1743–1748.
133. Rhoney DH, Parker D. Use of sedative and analgesic agents in neurotrauma patients: effects on cerebral physiology. Neurol Res. 2001;23:237–259.
134. Greher M, Sitzwohl C, Andel D, et al. A new concept of analgesia in severely burned patients based on the who guidelines for pain management. Anesthesiology. 2001;95:A384.
135. Campos LA, Soares LG, Fernandes MA, et al. Immediate postoperative analgesia and sedation following heart surgery: a comparative analysis of dexmedetomidine chlorohydrate versus remifentanyl hydrochloride. Crit Care. 5;(Suppl 3):70.
136. Meiser A, Laubenthal H. Inhalational anaesthetics in the ICU: theory and practice of inhalational sedation in the ICU, economics, risk-benefit. Best Pract Res Clin Anaesthesiol. 2005;19(3):523–538.
137. Enlund M, Wiklund L, Lambert H. A new device to reduce the consumption of a halogenated anesthetic agent. Anaesthesia. 2001;56(5):429–423.
138. Tempia A, et al. The anesthetic conserving device compared with conventional circle system used under different flow conditions for inhaled anesthesia. Anesth Analg. 2003;96:1056–1061.
139. Sackey PV, Martling CR, Radell PJ. Three cases of PICU sedation with isoflurane delivered by the ‘AnaConDa’. Paediatr Anaesth. 2005;15(10): 879–885.
140. Eger EI. The pharmacology of isoflurane. Br J Anaesth. 1984;56:71–99S.
141. Hirshman CA, Edelstein G, Peetz S, et al. Mechanism of action of inhalational anesthesia on airways. Anesthesiology. 1982;56:107–111.
142. Korenaga S, Takeda K, Ito Y. Differential effects of halothane on airway nerves and muscle. Anesthesiology. 1984;60:309–318.
143. Saulnier FF, Durocher AV, Deturck RA, et al. Respiratory and hemodynamic effects of halothane in status asthmaticus. Intensive Care Med. 1990;16:104–107.
144. Maltais F, Reissmann H, Navalesi P, et al. Comparison of static and dynamic measurements of intrinsic PEEP in mechanically ventilated patients. Am J Respir Crit Care Med. 1994;150:1318–1324.
145. Echeverria M, Gelb AW, Wexler HR, et al. Enflurane and halothane in status asthmaticus. Chest. 1986;89:152–154.
146. Padkin AJ, Baigel G, Morgan GA. Halothane treatment of severe asthma to avoid mechanical ventilation. Anaesthesia. 1997;52:994–997.
147. Gal TJ. Pulmonary mechanics in normal subjects following endotracheal intubation. Anesthesiology. 1980;52:27–35.
148. Habre W, Scalfaro P, Sims C, et al. Respiratory mechanics during sevoflurane anesthesia in children with and without asthma. Anesth Analg. 1999;89:1177–1181.
149. Phipps P, Garrard CS. The pulmonary physician in critical care • 12: acute severe asthma in the intensive care unit. Thorax. 2003;58:81–88.
150. Shoemaker WC, Belzberg H, Wo CC, et al. Multicenter study of noninvasive monitoring systems as alternatives to invasive monitoring of acutely ill emergency patients. Chest. 1998;114(6):1643–1652.
151. Bauer JJ, Schulam PG, Kaufman HS, et al. Laparoscopy for the acute abdomen in the postoperative urologic patient. Urology. 1998;51:917–919.
152. Fabian TC, Croce MA, Stewart RM, et al. A prospective analysis of diagnostic laparoscopy in trauma. Ann Surg. 1993;217:557–564.
153. Iberti TJ, Salky BA, Onofrey D. Use of bedside laparoscopy to identify intestinal ischemia in postoperative cases of aortic reconstruction. Surgery. 1989;105:686–689.
154. Berci G, Sachier JM, Paz Parlow M. Emergency laparoscopy. Am J Surg. 1991;161:332–335.
155. Ivatury RR, Simon RJ, Stahl WM. A critical evaluation of laparoscopy in penetrating abdominal trauma. J Trauma. 1993;34:822–827.
156. Forde KA, Treat MR. The role of peritoneoscopy (laparoscopy) in the evaluation of the acute abdomen in critically ill patients. Surg Endosc. 1992;6:219–221.
157. Walsh RM, Popovich MJ, Hoadley J. Bedside diagnostic laparoscopy and peritoneal lavage in the intensive care unit. Surg Endosc. 1998;12:1405–1409.
158. Gagne DJ, Malay MB, Hogle NJ, et al. Bedside diagnostic minilaparoscopy in the intensive care patient. Surgery. 2002;131(5):491–496.
159. Pecoraro AP, Cacchione RN, Sayad P, et al. The routine use of diagnostic laparoscopy in the intensive care unit. Surg Endosc. 2001;15:638–641.
160. Rosin D, Haviv Y, Kuriansky J, et al. Bedside laparoscopy in the ICU: report of four cases. J Laparoendosc Adv Surg Tech. 2001;11(5):305–309.
161. Plummer AL, Gracey DR. Consensus conference on artificial airways in patients receiving mechanical ventilation. Chest. 1989;96(1):178–180.
162. Stock MC, Woodward CG, Shapiro BA, et al. Perioperative complications of elective tracheostomy in critically ill patients. Crit Care Med. 1986;14(10):861–863.
163. Friedman Y, Fildes J, Mizock B, et al. Comparison of percutaneous and surgical tracheostomies. Chest. 1996;110(2):480–485.
164. Ciaglia P, Firsching R, Syniec C. Elective percutaneous dilatational tracheostomy. A new simple bedside procedure; preliminary report. Chest. 1985;87(6):715–719.
165. Mansharamani NG, Koziel H, Garland R, et al. Safety of bedside percutaneous dilatational tracheostomy in obese patients in the ICU. Chest. 2000;117(5):1426–1429.
166. Freeman BD, Isabella K, Lin N, et al. A metaanalysis of prospective trials comparing percutaneous and surgical tracheostomy in critically ill patients. Chest. 2000;118:1412–1418.
167. Ernst A, Garland R, Zibrak J. Percutaneous tracheostomy. J Bronchol. 1998;5:247–250.
168. Kluge S, Meyer A, Kuhnelt P, et al. Percutaneous tracheostomy is safe in patients with severe thrombocytopenia. Chest. 2004;126(2):547–551.
169. Hubner N, Rees W, Seufert K, et al. Percutaneous dilatational tracheostomy done early after cardiac surgery: outcome and incidence of mediastinitis. Thorac Cardiovasc Surg. 1998;46:89–92.
170. Westphal K, Byhahn C, Lischke V. Tracheostomy in intensive care. Anaesthesist. 1999;48:142–156.
171. Cantais E, Kaiser E, Le-Goff Y, et al. Percutaneous tracheostomy: prospective comparison of the translaryngeal technique versus the forceps-dilational technique in 100 critically ill adults. Crit Care Med. 2002;30:815–819.
172. Van Natta TL, Morris JA, Eddy VA, et al. Elective bedside surgery in critically injured patients is safe and cost-effective. Ann Surg. 1998;227:618–626.
173. Akinci IO, Ozcan P, Tugrul S, et al. Percutaneous endoscopic gastrostomy in the ICU. Ulus Travma Derg. 2000;6(4):281–283.
174. Russel RR, Brotman M, Norris F. Percutaneous gastrostomy—a new simplified and cost-effective technique. Am J Surg. 1984;148:132–137.
175. Campos AC, Marchesini JB. Recent advances in the placement of tubes for enteral nutrition. Curr Opin Clin Nutr Metab Care. 1999;2:265–269.
176. Jeffrey L, Ponsky MD, Michael WL, et al. Percutaneous endoscopic gastrostomy: indications, limitations, techniques, and results. World J Surg. 1989;13:165–170.
177. Wasljew BK, Ujlkl GT, Beal JM. Feeding gastrostomy; complications and mortality. Am J Surg. 1982;143:194–195.
178. Ferraro F, Capasso A, Troise E. Enteral nutrition in the ICU: clinical experience of percutaneous endoscopic gastrostomy. Riv Ital Nutr Parenter Enter Anno. 2004;22(2):86–90.
179. Carrillo E, Heniford B, Osborne D, et al. Bedside percutaneous endoscopic gastrostomy: a safe alternative for early nutritional support in critically ill trauma patients. Surg Endosc. 1997;11(11):1068–1071.
180. Dimick P, Helvig E, Heimbach D, et al. Anesthesia-assisted procedures in a burn intensive care unit procedure room: benefits and complications. J Burn Care Rehabil. 1993;14(4):446–449.
181. Gueugniaud PY. [Management of severe burns during the 1st 72 hours] [article in French]. Ann Fr Anesth Reanim. 1997;16(4):354–369.
182. Edrich T, Friedrich AD, Holger K. International Anesthesia Research Society critical care and trauma; ketamine for long-term sedation and analgesia of a burn patient. Anesth Analg. 2004;99:893–895.
183. Mayer SA, Claassen J, Lokin J, et al. Refractory status epilepticus frequency, risk factors, and impact on outcome. Arch Neurol. 2002;59:205–210.
184. Lothman E. The biochemical basis and pathophysiology of status epilepticus. Neurology. 1990;40(suppl 2):13–23.
185. Shorvon S. The management of status epilepticus. J Neurol Neurosurg Psychiatry. 2001;70(suppl II):ii22–ii27.
186. Coeytaux A, Jallon P, Galobardes B, et al. Incidence of status epilepticus in French-speaking Switzerland (EPISTAR). Neurology. 2000;55:693–697.
187. Holtkamp M, Masuhr F, Harms L, et al. The management of refractory generalised convulsive and complex partial status epilepticus in three European countries: a survey among epileptologists and critical care neurologists. J Neurol Neurosurg Psychiatry. 2003;74:1095–1099.
188. Rasmussen PA, Yang Y, Rutecki PA. Propofol inhibits epileptiform activity in rat hippocampal slices. Epilepsy Res. 1996;25:169–175.
189. Wood PR, Browne GPR, Pugh S. Propofol infusion for the treatment of status epilepticus. Lancet. 1988;I:480–481.
190. Brown LA, Levin GM. Role of propofol in refractory status epilepticus. Ann Pharmacother. 1998;32:1053–1059.
191. Stecker MM, Kramer TH, Raps EC, et al. Treatment of refractory status epilepticus with propofol: clinical and pharmacokinetic findings. Epilepsia. 1998;39:18–26.
192. Begemann M, Rowan AJ, Tuhrim S. Treatment of refractory complex-partial status epilepticus with propofol: case report. Epilepsia. 2000;41:105–109.
193. Prasad A, Worral BB, Bertram EH, et al. Propofol and midazolam in the treatment of refractory status epilepticus. Epilepsia. 2001;42:380–386.
194. Claassen J, Hirsch LJ, Emerson RG, et al. Treatment of refractory status epilepticus with pentobarbital, propofol, or midazolam: a systematic review. Epilepsia. 2002;43:146–153.
195. Rampton AJ, Griffin RM, Durcan JJ, et al. Propofol and electroconvulsive therapy. Lancet. 1988;I:196–197.
196. Rossetti AO, Reichhart MD, Schaller MD, et al. Propofol treatment of refractory status epilepticus: a study of 31 episodes. Epilepsia. 2004;45(7):757–763.
197. Parviainen I, Uusaro A, Kälviäinen R, et al. High-dose thiopental in the treatment of refractory status epilepticus in intensive care unit. Neurology. 2002;59:1249–1251.
198. Krishnamurthy KB, Drislane FW. Depth of EEG suppression and outcome in barbiturate anesthetic treatment for refractory status epilepticus. Epilepsia. 1999;40:759–762.
199. Sutherland MJ, Burt P. Propofol and seizures. Anaesth Intens Care. 1994;22:733–737.
200. Iwasaki F, Mimura M, Yamazaki Y, et al. Generalized tonic-clonic seizure induced by propofol in a patient with epilepsy. Masui. 2001;50:168–170.
201. Borgeat A, Dessibourg C, Popovic V, et al. Propofol and spontaneous movements: an EEG study. Anesthesiology. 1991;74:24–27.
202. Walder B, Tramèr MR, Seeck M. Seizure-like phenomena and propofol: a systematic review. Neurology. 2002;58:1327–1332.
203. Borgeat A. Propofol: pro- or anticonvulsant? Eur J Anaesth. 1997;14(suppl 15):17–20.
204. Modica PA, Tempelhoff R, White PF. Pro- and anticonvulsant effects of anesthetics (part II). Anaesth Analg. 1990;70:433–444.
205. Iwaku F, Otsuka H, Kuraishi H, et al. [The investigation of isoflurane therapy for status asthmaticus patients] [article in Japanese] Arerugi. 2005;54(1):18–23.
206. Allen J, Shirk MB. Sedation and paralysis in the MICU. Intensive Care Med. 1999;25:377–382.
207. Szem JW, Hydo LJ, Fischer E, et al. High-risk intrahospital transport of critically ill patients: safety and outcome of the necessary “road trip”. Crit Care Med. 1995;23:1660–1666.
208. Stearley HE. Patients' outcomes: intrahospital transportation and monitoring of critically ill patients by a specially trained ICU nursing staff. Am J Crit Care. 1998;7:282–287.
209. Corriere MA, Passman MA, Guzman RJ, et al. Comparison of bedside transabdominal duplex ultrasound versus contrast venography for inferior vena cava filter placement: what is the best imaging modality? Ann Vasc Surg. 2005;19:229–234.
210. Conners MS 3rd, Becker S, Guzman RJ, et al. Duplex scan-directed placement of inferior vena cava filters: a five-year institutional experience. J Vasc Surg. 2002;35:286–291.
211. Neser RA, Filho MC, de Oliveira Homa CM. Placement of inferior vena cava filter guided by ultrasound: report of two cases. J Vasc Br. 2006;5(1):71–73.
Appendices Sedation and Pain Scales
|
Appendix 40.1 Sedation/Agitation Scale |
|||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||
|
Appendix 40.2 Pain Intensity Scale |
|||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||