Ikram U. Haque
Andrea Gabrielli
Arno L. Zaritsky
Cardiopulmonary resuscitation (CPR) is described as a series of assessments and interventions performed during a variety of acute medical and surgical events where death is likely without immediate intervention. Among these events, sudden cardiac arrest (SCA) is a leading cause of death in the United States (1) and Canada (2) in adults. Cardiac arrest (CA) is defined as “cessation of cardiac mechanical activity as confirmed by the absence of signs of circulation.” As its name implies, in the prehospital arena, adult SCA is most commonly due to ventricular fibrillation (VF) (3) secondary to ischemic heart disease; asystole and pulseless electrical activity (PEA) are less common initial rhythms with SCA, although these rhythms may represent the initial identified rhythm in adults who actually experienced an acute VF or ventricular tachycardia (VT) event. Although VF and VT are considered to be the most common out-of-hospital (OOH) arrest rhythms, only 20% to 38% of in-hospital arrest patients have VF or VT as their initial rhythm. In contrast, children and young adults require CPR most commonly for respiratory arrest, airway obstruction, or drug toxicity. VF/VT is identified as the initial rhythm in 5% to 15% of OOH arrests in children (4). Other conditions such as trauma, external or internal hemorrhage, and drowning may call for resuscitation at any age.
Regardless of the cause, immediate and effective CPR can save lives. In patients with witnessed VF CA, CPR doubles (3) or triples (5) the rate of survival. Unfortunately, only ~27% of OOH arrest victims receive bystander CPR.
The primary goal of CPR is to generate sufficient oxygen delivery to the coronary and cerebral circulations in order to maintain cellular viability while attempting to restore a perfusing cardiac rhythm by defibrillation, pharmacologic intervention, or both.
Immediate Concerns
Effective CPR can be performed by following a few basic rules:
· Immediately assess the environment for danger and move the patient if necessary. Never assume that an environment is safe.
· Minimize the time from cardiac arrest recognition to starting effective CPR. For every minute without CPR during witnessed VF CA, survival decreased by 7% to 10% in contrast to a decrease in survival by 3% to 4% per minute when bystander CPR preceded attempted defibrillation (6).
· Defibrillate immediately if a defibrillator is rapidly available (<3–5 minutes) in patients with VF. This should be the primary treatment focus within the first few minutes of SCA due to ventricular fibrillation. For each minute delay in defibrillation, chances of eventual hospital discharge decreased by 8% to 10% (7). Note that if the time from arrest to emergency medical service (EMS) arrival and initiation of CPR is more than 5 minutes, provision of 2 minutes of CPR before attempted defibrillation was associated with improved outcome (8,9).
· “Push hard and fast” during chest compressions and minimize the duration of interruptions to reassess the patient's rhythm. It is recommended to interrupt chest compressions only briefly and about every 2 minutes to assess the rhythm and switch rescuer if feasible.
· While CPR is in progress, attempt to identify the cause of arrest. Although the steps of CPR are uniform, other resuscitation interventions may be indicated based on the cause of CA. If the patient fails to respond to standard CPR interventions, think about delayed recognition and recall the H's and T's (Table 46.1) to help identify a potentially correctable cause for ongoing cardiac arrest.
· Good teamwork increases the effectiveness of resuscitation when more than one rescuer is available.
· Attention to postresuscitation care is an important element of neurologic outcome. Focus on restoring and supporting adequate cardiac output and tissue perfusion, monitor and maintain normal blood glucose concentrations, treat the underlying cause of the arrest, maintain normothermia, and consider therapeutic hypothermia to maximize survival and cerebral recovery.
· If the patient fails to respond to effective CPR, appropriate judgment is needed in determining when to stop resuscitative efforts.
|
Table 46.1 Potential correctable problems during cardiac arrest: “6 H's and 5 T's” |
||
|
Guidelines for CPR and advanced adult and pediatric advanced life support are published every 5 years by the American Heart Association (AHA) (10). These guidelines are based on an extensive evidence-based review by national and international experts leading to the publication of a consensus on science and treatment recommendations prepared by the International Liaison Committee on Resuscitation (ILCOR) (11,12). ILCOR is a collaborative organization of American, European, Australian, Canadian, South African, and Latin American resuscitation councils with the goal of identifying the best resuscitation evidence (13).
Outcome of Cardiopulmonary Resuscitation
Measuring Outcome after Cardiac Arrest
Retrospective and prospective observational outcome reports have been published about the success rates of both in-hospital and out-of-hospital cardiac arrest, but most of these are single-center reports with relatively few subjects. More recently, cardiac arrest events and outcomes have been systematically monitored in large multicenter settings. To facilitate data comparison across communities, international guidelines were published for data collection using standard definitions of events and outcome for both adults and children (the Utstein Guidelines) (14,15,16). In 2000, the AHA established a National Registry of Cardiopulmonary Resuscitation (NRCPR) to systematically collect data on the epidemiology, processes of care, and outcome of in-hospital CPR (4,17). This comprehensive database has, at the time of this writing, an excess of 100,000 cardiac arrest events and provides important insights into the mechanism, logistics, and outcomes of cardiac arrest and helps evaluate the impact of interventions such as a rapid response team. The standard consensus terms used to describe outcome of CA are as follows (13):
1. Successful defibrillation: Termination of fibrillation to an organized electrical rhythm (including PEA for at least 5 seconds after shock delivery).
2. Return of spontaneous circulation (ROSC): Restoration of a spontaneous perfusing heart rhythm in the absence of external chest compressions for approximately >30 seconds. This term is not applicable when extracorporeal support is used, such as extracorporeal membrane oxygenation or a biventricular assist device.
3. Survived event:
a. Out-of-hospital setting: Sustained ROSC with spontaneous circulation until admission and transfer of care to medical staff at the receiving hospital.
b. In-hospital setting: Sustained ROSC for >20 minutes (or support of circulation if extracorporeal circulatory support is applied).
4. End of event: A resuscitation event is deemed to have ended when either death is declared or spontaneous circulation is restored and sustained for 20 minutes or longer. If extracorporeal life support is being provided, the end of event is 20 minutes after the establishment of extracorporeal circulation.
5. Survival to hospital discharge: Survival to hospital discharge is the point at which the patient is discharged from the hospital acute care unit regardless of neurologic status, outcome, or destination.
6. Neurologic outcome at discharge: Assessment of neurologic recovery is measured at discharge in terms of recovery of consciousness and achievement of precardiac arrest level of functioning.
Out-of-hospital Cardiac Arrest
Despite improvement in the scientific basis for resuscitation practices and extensive efforts at CPR training of lay and professional rescuers over the years, the outcome of most adult victims of out-of-hospital cardiac arrest remains poor, with a median reported survival to hospital discharge of 6.4% (7,18). A recent study suggested that adults who had a cardiac arrest in a public location (i.e., witnessed) were more likely to arrive to the hospital alive (39% vs. 31%, p = 0.049) and were more likely to have a good neurologic outcome after 6 months (35% vs. 25%, p = 0.023) compared with patients who had a cardiac arrest in a nonpublic location (19).
In children, the epidemiology and physiology of OOH cardiac arrest is different. In this group of patients, a recent systematic review of 41 studies of out-of-hospital cardiac arrest, including trauma, revealed an ROSC of 30%, with survival to admission of 24% but survival to discharge of 12% and neurologically intact survival of only 4% (20). The initial cardiac rhythms observed in these children were asystole, 78%; PEA, 12.8%; VF/pulseless VT, 8.1%; and bradycardia with a pulse, 1%.
In-hospital Cardiac Arrest
Despite efforts to train professional in-hospital rescuers to deliver effective CPR and use various devices and therapeutic drugs during resuscitation, the objective survival rates over the years have hardly changed (21,22). Currently, in-hospital cardiac arrest in adults has an overall survival of about 18% (17,23,24,25). Analysis of data from the NRCPR found that the prevalence of VF or pulseless VT as the first documented pulseless rhythm during in-hospital cardiac arrest was only 23% in adults and 14% in children (4). The prevalence of asystole as the initial rhythm was 35% in adults and 40% in children, whereas the prevalence of PEA was 32% versus 24% in adults and children, respectively. The rate of survival to hospital discharge following pulseless cardiac arrest was higher in children than adults, 27% versus 18%, respectively. Of these survivors, 65% of children and 73% of adults had good neurologic outcome. After adjusting for known predictors, such as arrest location and monitoring at time of arrest, outcome was surprisingly worse when the rhythm was VF/VT in children compared with asystole and PEA (4). Further analysis of these data showed that VF/VT occurred during CPR in children more commonly than it occurred as the initial rhythm (26). Survival to discharge is highest (35%) when VF/VT is the initial rhythm compared with much worse survival (11%) if this rhythm develops during resuscitation (26).
Neurologic Outcome
Neurologic outcome is determined by the cause of arrest (e.g., degree of shock or hypoxemia prior to arrest), the duration of no flow, adequacy of flow during CPR, restoration of adequate flow following ROSC, and subsequent injury secondary to postarrest management such as the occurrence of hyperthermia or hypoglycemia. Survivors who ultimately have a good outcome generally awaken within 3 days after CA. Most patients who remain neurologically unresponsive due to anoxic-ischemic encephalopathy for more than 7 days will fail to survive, and those who do survive often have poor neurologic recovery (27,28,29). Neurocognitive impairment ranges from dependency on others for care to remaining in a minimally conscious or vegetative state. Achieving good functional outcome is the ultimate goal for successful CPR because survival with severe neurologic injury is a terrible cost to patients, their family members and friends, and society at large. The financial implications of caring for these patients with disordered consciousness are substantial (30).
Unfortunately, most studies reporting outcome data lack these difficult-to-obtain elements or have used crude methods to describe neurologic outcome, such as the composite scores from the Glasgow outcome scale (GOS) (31) and Cerebral Performance Category (CPC) (32,33). One important limitation of these scales is the possibility of wide variation of neurologic function for the same score. In children, other scales such as the Pediatric Cerebral Performance Category (PCPC) and Pediatric Overall Performance Category (POPC) have been used (34,35,36). Currently, 11% to 48% of CA patients admitted to the hospital will be discharged with good neurologic outcome (21,37,38). Recent data from the NRCPR show that neurologic outcome in discharged adult survivors is generally good with 73% of patients with Cerebral Performance Category 1 (17).
Initial Considerations
CPR is primarily based on two principles:
1. Providing artificial ventilation and oxygenation through an unobstructed airway to maintain gas exchange. Since cardiac output is limited, the rescuer needs to avoid ventilation in excess of that required for adequate ventilation/perfusion matching.
2. Delivering chest compressions to maintain threshold blood flow, especially to the heart and brain, while minimizing interruption of compressions.
Basic Life Support
Basic life support (BLS) is the initial phase of CPR recognized as the “ABCs” of CPR: A, airway; B, breathing; C, circulation. Effective BLS can provide almost 30% of normal cardiac output with adequate arterial oxygen content; this is sufficient to protect the brain for minutes until effective defibrillation or other definitive therapeutic maneuvers are provided (39). With the 2000 guidelines for CPR, a new evidence-based approach to ventilation during CPR was introduced that continued with the 2005 edition. New evidence from laboratory and clinical science led to a de-emphasis on the role of ventilation following a dysrhythmic cardiac arrest (arrest primarily resulting from an acute cardiovascular event, such as ventricular fibrillation or tachycardia) (40). However, after asphyxial cardiac arrest (cardiac arrest primarily resulting from respiratory arrest and less commonly from shock), the traditional emphasis on ensuring airway patency, effective ventilation, and circulation remains fundamental to achieving survival and the intact neurologic outcome of patients. The following section summarizes BLS in adults; differences in BLS for infants and children compared with adults are seen in Table 46.2.
Airway
After establishing unresponsiveness and calling for help, opening the airway and maintenance of airway patency are the next steps of CPR. Provision and maintenance of a patent upper airway should be provided with the maneuvers listed below. These maneuvers are described in detail in basic airway management chapters.
|
Table 46.2 Summary of basic life support ABCD maneuvers for infants, children, and adults for lay rescuers and health care providers (newborn information not included) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
1. Head tilt/chin lift
2. Jaw-thrust maneuver
3. Triple airway maneuver
4. Mandibular forward displacement
If airway obstruction is felt to be present and foreign body is suspected, immediate removal should be done using basic airway management guidelines.
Breathing
Determination of Apnea
There are several recommended methods of determining the absence of spontaneous breathing in an unconscious patient when no pulse oximetry is present. Spontaneous respiration may be difficult to observe unless the airway is opened (41). Once airway patency is established, the rescuer should place his or her ear over the victim's mouth and nose. The rise and fall of the chest should be noted while listening for breath sounds and feeling for expired air. The absence of these signs is indicative of apnea. Frequently, gasping, gurgling, snoring sounds or agonal respiratory efforts may be observed during sudden cardiac arrest, especially within the first few minutes of collapse. This is typically not sustained, and should not be mistaken for adequate spontaneous respiration. In some instances, the victim may exhibit respiratory efforts but no air exchange is observed. This indicates severe upper airway obstruction; opening the airway will facilitate the resumption of air movement. Despite the widespread diffusion of these recommendations, studies showed that lay rescuers as well as professional rescuers are unable to accurately determine adequate breathing in unresponsive patients (42,43). Currently, it is recommended that if breathing cannot be confirmed within 10 seconds, two rescue breaths should be given.
Initiation of Rescue Breathing
If the patient is not breathing, immediate rescue breaths are delivered using the maneuver appropriate for the situation. Most first-responder personnel and medical professional staff in hospitals are trained to use adjunct devices during BLS. When a bag-mask ventilation (BMV) is not immediately available, mouth-to-mouth rescue breathing can still be life saving.
Intuitively, the presence of vomitus and fear of infectious contamination can affect the willingness of rescuers to perform mouth-to-mouth resuscitation. Lawrence and Sivaneswaran showed that only 13% of 70 hospital staff members surveyed would use mouth-to-mouth ventilation during CPR and 59% would prefer to do mouth-to-mask ventilation (44). Specialized breathing masks with a one-way valve can be utilized during CPR. The valve prevents the exhaled air from entering the rescuer's mouth.
During both one and two-rescuer CPR, two mouth-to-mouth breaths are given during a pause after every 30th chest compression. This ratio is the same for adults, children, and infants when there is only one rescuer. If two or more professional rescuers are present, a 15:2 ratio is used in children (defined as child if there are no signs of puberty such as facial hair or breast development) and infants.
Once an advance airway (i.e., endotracheal tube, laryngeal mask airway [LMA], or pharyngotracheal Combitube) is obtained, chest compressions are given continuously at a rate of 100 compressions per minute without interruption for ventilation. A ventilation rate of eight to ten can sufficiently match the perfusion achieved by chest compression (20%–30% of normal at best) (45). Rescue breathing when there is a pulse should not exceed 12 breaths/minute (45).
Manual Resuscitators (Bag-valve Devices)
Bag-valve devices (BVDs) of various designs and sizes are available for adults and children to deliver manual breaths. A self-inflating, manually operated bag with a nonrebreathing valve is preferred because it allows ventilation even if there is no connection to an oxygen source. This device may be used in conjunction with a face mask, endotracheal tube, or other invasive airway device.
The standard parts of a BVD include (a) a delivery port with a 15-mm/22-mm adapter coupling that can be connected to the mask or tracheal tube; (b) a one-way, non jam valve that allows a minimum of 15 L/minute oxygen flow rate for spontaneous and controlled ventilation; and (c) a system for ensuring delivery of a high oxygen concentration through an auxiliary oxygen inlet at the back of the bag or by an oxygen reservoir. The bag holds a volume up to 1,600 mL. Some pediatric resuscitator bags are provided with a 25- to 30-cm H2O pop-off valve to avoid excessive positive airway pressure, thereby reducing the risk of gastric insufflation and hyperinflation of the lungs and subsequent pulmonary barotrauma, but a pop-off valve is not recommended during CPR in adults since higher airway pressures may be needed to achieve adequate ventilation. A malfunctioning valve may lead to improper venting and inadequate ventilation. This can be recognized by the sound of air escaping through the relief valve while squeezing the bag. Adjusting or partially occluding a malfunctioning valve may be life saving.
The operator should be positioned at the top of the victim's head. Appropriate face mask size should be selected, the airway opened, and a tight seal created covering the mouth and the nose as described previously. After proper head positioning, the bag is squeezed to deliver the breath over 1 second. Tidal volume is sufficient if visible chest rise is present. An oropharyngeal airway or nasopharyngeal airway may be used to facilitate bag-mask ventilation in case of upper airway obstruction. Proper bag-mask ventilation requires training, practice, and familiarity with the equipment.
A single rescuer may have difficulty maintaining a correct head position and delivering adequate tidal volume at the same time (46,47,48). Thus, two rescuers may be more effective where one rescuer seals the mask to the mouth, performs a jaw thrust, and maintains head extension while the other rescuer squeezes the bag with both hands (49). Oxygen supplementation during bag-mask ventilation delivers 40% to 60% O2 without an oxygen reservoir and over 90% with an oxygen reservoir (50,51).
Complications associated with the use of a bag-mask device are primarily due to excessive ventilating pressures causing pneumothorax, pneumomediastinum, and gastric distention that can lead to decreased total lung compliance, regurgitation, and gastric rupture (52). Unless the rescuer is proficient in the use of flow-inflating devices (e.g., Mapleson D system, typically used by anesthesia personnel) during CPR, it is preferable to use a self-inflating handheld resuscitator bag.
Special consideration should be applied for pediatric patients. In fact, the pediatric airway may be flattened by excessive extension of the cervical spine during the head tilt–chin lift maneuver. Smaller breaths must be used to avoid abdominal distention, regurgitation, and pulmonary barotrauma. As with adults, appropriate tidal volume is characterized by visible chest rise.
Oxygen-powered, Manually Triggered Ventilation Devices
Oxygen-powered breathing devices may be used when available during CPR. These simple ventilatory devices require high oxygen flow rates to overcome air leak (44). Although they may be able to deliver adequate tidal volumes, high-flow-rate time-cycled oxygen-powered devices carry a risk of severe gastric distention when used with a face mask.
Inspiratory Impedance Valve
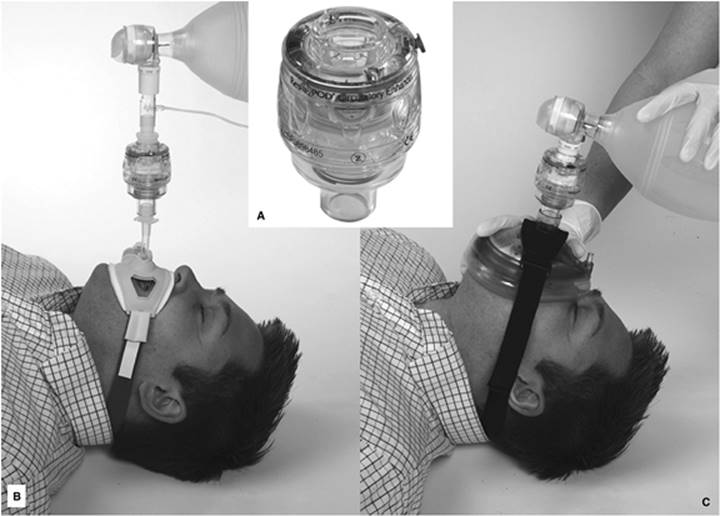
A small inspiratory impedance valve device was recently introduced to occlude the airway selectively during the decompression phase of chest compressions without interfering with exhalation or resuscitation bag ventilation. This device, as shown in Figure 46.1, is placed between the end of an endotracheal tube or face mask and the resuscitation bag, which then limits air entry into the lungs during chest recoil or when the patient spontaneously breathes. In the latter circumstance, the patient needs to overcome the inspiratory threshold pressure for air flow to occur. The resulting modest reduction in intrathoracic pressure enhances venous return to the heart between chest compressions and thus cardiac output. This device has no deleterious effect on ventilation, and can enhance coronary and cerebral blood flow during CPR in animals and humans along with a higher rate of ROSC after defibrillation (53,54). An enhancement of cardiac output during spontaneous ventilation has also been observed in hypovolemic shock states (55). In spite of the favorable hemodynamic effect, the use of this device so far has not demonstrated a definitive long-term neurological improvement after ROSC. At the time of this writing, a large multicenter clinical trial is under way.
|
|
|
Figure 46.1. Top center (A) showing an inspiratory impedance valve device (ResQPOD, Advanced Circulatory Systems, Inc., Minneapolis, MN). The device is applied between the resuscitation bag and endotracheal tube as shown in bottom left (B) or between the resuscitation bag and face mask as shown in bottom right (C). (Pictures courtesy of ResQPOD, Advanced Circulatory Systems, Inc., Minneapolis, MN.) |
Circulation
Determination of Circulation
In the absence of a continuous arterial line monitoring, palpation for carotid or femoral pulses has been traditionally the gold standard for a diagnosis of cardiac arrest. Recent studies, however, showed that both lay rescuers (56) and health professionals are unable to accurately determine the presence or absence of a pulse; most required more than the recommended 10 seconds to feel confident about whether a pulse was present (42,57). Based on this observation that can significantly delay chest compression, the pulse check was eliminated for lay rescuers and de-emphasized for health professionals in the 2000 and 2005 guidelines (45,58), where verification of “no pulse” is not recommended beyond 10 seconds.
Mechanism of Blood Flow during Chest Compression
In the early 19th century, open cardiac massage was used successfully by Kristian et al. in the emergency treatment of cardiac arrest (59). In a short time, this became the method of choice for CPR (60,61), with variable outcomes reported. Open cardiac massage requires a thoracotomy and the heart is squeezed directly by the hands of the rescuer (61,62). The basic idea was to produce an effective perfusion pressure gradient for blood flow from the heart to vital organs. Open cardiac massage has been utilized in a variety of special situations where the access to the chest is immediately feasible (63,64,65,66). For example, in the cardiac intensive care unit (ICU), open cardiac compression is used both in adult and pediatric patients in the immediate postoperative setting (67). Outside of the operating room (OR), the use of open cardiac massage, although it improved coronary perfusion pressure and increased ROSC, was not followed by improved survival (68).
In 1960, Kouwenhoven et al. reported successful resuscitation of dogs and subsequently humans with ventricular fibrillation cardiac arrest using the combination of closed chest compression, artificial respiration, and electrical defibrillation (69,70). They hypothesized that the heart was physically squeezed between the sternum and vertebral column, whereby the blood flow generated is similar to the mechanism of spontaneous contraction of the heart; hence, this is called the “cardiac pump” model. This model, however, does not explain several clinical observations in contrast with the cardiac pump theory such as the ineffectiveness of CPR during flail chest, although theoretically it should be easier to compress the heart in this condition, or the effectiveness of closed chest CPR in patients with hyperinflated chest due to severe emphysema.
The cardiac pump model was challenged in the 1970s when Criley et al. reported ROSC with cough during ventricular fibrillation (71,72). In 1980, Rudikoff et al. reported that fluctuations of intrathoracic pressures were primarily responsible for blood flow during CPR (73,74). These findings supported a noncardiac or “thoracic pump” mechanism for blood flow during CPR. This model proposes that increased intrathoracic pressure during chest compression elevates the pressure of blood located in structures within the thorax, creating the gradient for forward blood flow from the intrathoracic to lower pressure extrathoracic arteries. During relaxation, intrathoracic pressure drops, resulting in refilling of the heart with blood. In this model, the heart acts as a passive conduit. Echocardiographic studies to elucidate the pumping mechanism during cardiac arrest have failed to resolve the controversy (75,76,77). It appears that in adults with thin chest walls, direct cardiac compression does occur, whereas in prolonged resuscitation and in patients with thick chest walls or hyperinflated lungs, the thoracic pump mechanism becomes the predominant flow mechanism. It is also likely that both mechanisms are involved in some cases.
In infants and children, a mechanism of direct cardiac compression is well supported by the observation of CPR performed in young animal models (78). Currently, closed chest compression is the standard method of producing blood flow during CPR for both adult and pediatric victims.
Closed Chest Compression
Closed chest compressions consist of the rhythmic application of pressure over the lower half of the sternum. Even if properly performed, in adults, chest compressions can only produce systolic arterial pressures of 60 to 80 mm Hg; diastolic pressure is usually low and mean arterial pressure in the carotid artery seldom exceeds 40 mm Hg (79). These values are low compared to normal but still can provide critical blood flow to the heart and brain while attempts to restore definitive cardiac activity are implemented. To achieve maximum benefit from chest compressions during CPR, attention should be given to the following components:
1. Positioning the patient: The victim should lie supine on a hard surface. If the patient is on a soft bed, then place a backboard beneath the patient (80). The rescuer should kneel beside the victim's thorax if the victim is on the floor (81), or adjust the bed to the level of the rescuer's hip if the victim is on a bed. Other positions like over-the-head CPR and two-person straddle CPR are described, but the efficacy of these techniques has not been established (82).
2. Positioning of rescuer hands: In adults, the rescuer ideally should compress the lower half of the victim's sternum. Locating proper hand position, however, has been confusing in lay rescuer education, so it is easier to teach that the rescuer should place the heel of the hand on the sternum in the center (middle) of the chest between the nipples and then place the heel of the second hand on top of the first so that the hands are overlapped and parallel (83,84). Compressions are delivered while keeping the arms straight at elbow. This is best achieved by leaning over the victim, which allows the rescuer's weight to be used in producing effective chest compression, but the rescuer should avoid maintaining compression on the chest during the relaxation phase, since this impairs venous return (85,86).
In children, the rescuer again should ideally compress the lower half of the sternum, avoiding the xiphoid process and the ribs, but the lay rescuer is taught to position the heel of one hand at the midnipple line. Either one or two hands can be used in children, depending on the strength of the rescuer. In a child, the use of two hands generates higher compression pressures compared with one hand and is less fatiguing in a manikin study (87), but no outcome study has shown superiority of one method over the other.
In infants, two different techniques are used: The two-finger technique and the two-thumb encircling technique. With the two-finger technique, the rescuer compresses the lower half of the sternum just below the intermammary line with the second and third or third and fourth fingers (78,88,89,90). This is the only technique to be used by lay rescuers. The two-thumb encircling hands technique is recommended when there are two health care provider rescuers. The infant's chest is encircled with both hands with the thumbs placed on the lower half of the sternum and the fingers spread around the thorax. Compression is delivered with both thumbs while the lateral chest is squeezed simultaneously with the fingers. The two-thumb encircling technique produces more consistent compression depth and higher coronary perfusion pressures (91,92,93).
3. Depth of compression: The sternum is depressed approximately 1½ to 2 inches (approximately 4 to 5 cm) in adults. In children and infants, the chest should be compressed to achieve one-half to one-third the depth of the anterior-posterior diameter of the chest. The higher proportional depth of compression is appropriate in infants, whereas one-third the depth of compression is appropriate in children. Data in manikin models show that rescuers often do not sustain an adequate depth of compression during CPR for more than 2 minutes. In studies of adults undergoing CPR in both the out-of-hospital (94) and in-hospital (95) setting, inadequate compression depth is commonly observed. Since adequate depth of compression is important in achieving optimal forward flow, emphasis should be placed on compressing “hard” as well as fast enough, and the rescuer performing chest compressions should change approximately every 2 minutes during the time when the patient's rhythm is being reassessed.
4. Compression rate: Recent studies in animals (96) and in humans (97,98) support that a rate of at least 80 per minute should be achieved to provide optimal forward blood flow during CPR, with some experts suggesting higher cardiac output with compression rates up to 150 per minute. Higher compression rates, however, are more difficult to sustain. It is important to remember that the compression rate refers to the speed of compressions, not the actual number of compressions delivered per minute. The actual number of chest compressions delivered per minute is determined by the rate of chest compressions and the number and duration of interruptions to open the airway, deliver rescue breaths, and time for analysis of cardiac rhythm and delivery of shock. To maximize the beneficial effects of chest compressions producing blood flow, the 2005 guidelines recommend compressions at a rate of approximately 100 per minute with interruptions in chest compressions kept to a minimum.
5. Decompression: After achieving the maximum depth of compression, the chest should be released to recoil on its own. It is crucial to let the chest recoil completely before the next compression is started. Incomplete chest recoil leaves residual positive (relative to atmospheric) intrathoracic pressure that decreases both coronary and cerebral perfusion (86).
6. Duty cycle: Duty cycle refers to the sum of the time interval from the start of compression until maximum compression is achieved (i.e., “compression cycle”) plus the time interval from the maximum compression to complete decompression (i.e., “decompression cycle”) prior to the next compression. Studies in animals and in manikin models showed that coronary and cerebral perfusion directly increased with increasing compression rate up to 130 to 150 per minute using a compression cycle between 20% and 50% of the duty cycle (99,100). Current guidelines recommend a 50% compression cycle (101).
Compression-to-Ventilation Ratio during Basic Life Support
Different compression-to-ventilation (C:V) cycles were recommended when one or two rescuers are present. In children, additional ratios were used to provide more ventilation. Recent studies show that both lay and health care rescuers provide poor chest compressions (94,95), and there is often a prolonged hands-off period during CPR while breaths are being given or the rhythm is being assessed, resulting in no cardiac output. Both animal data and theoretic models suggest that higher cardiac output will be achieved using a higher ratio of chest compressions and fewer interruptions for ventilation. The latter is acceptable since the overall cardiac output is only 25% to 30% of normal at best, which means that ventilation only needs to be 25% to 30% of normal to achieve adequate matching of ventilation to cardiac output during CPR. Therefore, the new guidelines recommend one universal ratio of 30 compressions to two ventilations in adults, children, and infants with one rescuer. If two health professionals are present, they should use a 15:2 ratio in children and infants. This approach maximizes chest compressions and minimizes time for ventilation, rhythm analysis, and shock, and improves ROSC and outcome (9,102).
In addition to being easy to teach and recall, the 30:2 compression:ventilation rate is designed to reduce the likelihood of hyperventilation, which impairs venous return as shown in a well-done animal study (103). Additionally, other data suggest that no ventilation is needed for the first few minutes of sudden cardiac arrest and need for initial ventilations has remained a matter of debate (9).
As previously noted, when the airway is secured, continuous chest compressions should be delivered continuously in an asynchronous mode with the ventilation. Unfortunately, the by-product of increasing the speed of chest compression is fatigue, detected by both animal (104) and human studies (105).
Acceptable Variations of Closed Chest Compressions
1. Interposed abdominal compression. The interposed abdominal compression (IAC) CPR technique uses a dedicated second rescuer to provide manual compression of the abdomen (midway between the xiphoid and the umbilicus) during the relaxation phase of chest compression. The purpose is to enhance venous return during CPR (106,107). When IAC CPR performed by trained providers was compared with standard CPR for in-hospital cardiac arrest, IAC CPR improved ROSC and short-term survival in two randomized trials and improved survival to hospital discharge in one study (108,109). The implementation of this technique is limited by the extensive complex training needed and the need for at least three rescuers to provide coordinated compressions and ventilation.
2. Active Compression-decompression. Active compression-decompression CPR (ACD CPR) is performed with a handheld device equipped with a suction cup to actively lift the anterior chest during decompression. It is thought that decreasing intrathoracic pressure during the decompression phase enhances venous return to the heart. Although substantial animal data demonstrated that the device improves cardiac output during CPR, clinical trials reported mixed results, with some showing improved survival (110,111,112) and others finding no effect when compared to standard CPR (113,114,115,116). The reason for the disparate results is not clear, but some data suggest that extensive training is required to use this device effectively, and there is a higher rate of rescuer fatigue from the increased effort required during both compression and relaxation. At the time of this writing, no ACD CPR device is approved by the Food and Drug Administration (FDA) for sale in the United States.
3. Phased thoracic-abdominal compression-decompression. This technique is essentially a combination of the IAC CPR and ACD CPR techniques described above. A handheld device is used to alternate chest compression and abdominal decompression with chest decompression and abdominal compression. The utility of this technique is also limited by the need for a dedicated rescuer and the complexity of training (117).
Mechanical Adjuncts for Circulation
1. Mechanical piston device. This device is composed of a plunger mounted on a backboard, which is driven by compressed gas to depress the sternum. The rate and depth of compressions is adjustable with a 50% compression cycle. Use of this device resulted in improved end-tidal CO2 in both in-hospital and out-of-hospital settings (118,119,120). The expense and bulkiness of the device has limited its widespread distribution and use.
2. Vest device (load distributing band). The load-distributing band (LDB) is a circumferential chest compression device composed of a pneumatically or electrically actuated constricting band and backboard. The band is wrapped around the patient and compresses the entire chest, producing thoracic pump CPR. Use of this device improved survival to emergency department arrival in one study (121); an FDA-approved device (AutoPulse) is available. A cohort study conducted before and after introduction of the load-distributing band found an improved rate of ROSC and survival to hospital discharge (122), whereas a randomized multicenter trial reported at the same time found no survival benefit 4 hours after the arrest and a lower rate of survival to hospital discharge (123).
Advanced Life Support
Advanced life support (ALS) entails advanced airway management including use of ancillary equipment to support ventilation and oxygenation, prompt recognition, and, when appropriate, treatment of life-threatening arrhythmias using electrical therapy including defibrillation, cardioversion, pacemaker insertion, and pharmacologic therapy. ALS includes the use of pharmacologic therapy and advanced procedures extending into the postarrest setting such as the use of therapeutic hypothermia.
Advanced Airway Management
Tracheal Intubation
Endotracheal intubation is indicated when the rescuer is unable to adequately ventilate or oxygenate the arrested or unconscious patient with bag-mask ventilation, or if prolonged ventilation is required and airway protective reflexes are absent in the patient with a perfusing rhythm. A properly placed endotracheal tube (ET) is the gold standard method for securing the airway. It maintains a patent airway to deliver effective positive pressure ventilation and use of positive end-expiratory pressure when indicated. It possibly reduces the risk from aspiration, especially if a cuffed tube is used, and it provides a means to suction airway secretions and provides an alternate route for resuscitation drugs delivery (124). No randomized adult studies have compared the outcome from endotracheal intubation to bag-mask ventilation, but one prospective randomized controlled trial in children showed no survival benefit of endotracheal intubation over bag-mask ventilation by trained EMS personnel (125).
Attempted endotracheal intubation by less skilled rescuers results in complications. Retrospective studies reported a 6% to 14% incidence of misplaced or displaced ETs (126,127,128). To minimize the risk of esophageal intubation, it is important to use an end-tidal CO2 (ETCO2) detector or esophageal detector device in addition to careful auscultation and observing symmetric chest rise. In patients requiring movement, exhaled CO2 monitoring (capnography) is helpful to detect tube displacement. Proper tube position should be confirmed by chest radiography when feasible. The intensivist is expected to master endotracheal intubation. However, expert personnel may not be immediately available in the ICU. Due to the technical difficulty and skill level needed for endotracheal intubation, there is increased emphasis on learning bag-mask ventilation, which could be used primarily for ventilation and can serve as rescue backup if attempted endotracheal intubation fails.
Confirmation of Correct Endotracheal Tube Placement
Clinical signs used to confirm correct ET placement are (a) visualization of bilateral chest rise, (b) bilateral breath sounds over the lateral lung fields, (c) absent breath sounds over the epigastrium, and (d) presence of water vapor/mist in the tube. None of these signs is confirmatory, however, and an ETCO2 detector or esophageal detector is indicated to confirm correct tube placement.
ETCO2 detector device
A disposable colorimetric device that detects ETCO2 has been investigated as a guide to correct endotracheal tube placement (129,130,131). The device fits on the end of the ET and is normally purple in color; exhaled CO2 turns the color to bright yellow indicating that the ET is in the trachea. The positive predictive value of this device for correct tube placement is close to 100%, but the negative predictive value ranges from 20% to 100% depending on whether the patient has a perfusing rhythm (132). False-negative results are seen if there is no or very low pulmonary blood flow, such as during cardiac arrest or with a large pulmonary embolus. Conversely, false-positive (i.e., the detector remains yellow) results are seen when it is contaminated with an acidic drug (e.g., epinephrine) or gastric contents. Currently, it is recommended to confirm each endotracheal intubation with an ETCO2 capnograph or an esophageal detector device. If doubt exists about whether the tube is correctly placed, direct visualization of the larynx is advised.
Esophageal detector device
There are two versions: The bulb and the syringe esophageal detector devices (EDD). The bulb EDD consists of a bulb that is compressed and attached to the endotracheal tube. When the squeezed bulb is released, if the tube is in the esophagus, the suction collapses the lumen of the esophagus or pulls the esophageal tissue against the tip of the tube, and the bulb will not re-expand (positive result for esophageal placement). The syringe EDD consists of a syringe attached to the ET; the rescuer attempts to pull the plunger of the syringe. If the tube is in the esophagus, it will not be possible to pull out the plunger (i.e., aspirate air) with the syringe. This device has high sensitivity for esophageal placement of ETs in both cardiac arrest and patients with a perfusing rhythm (133,134,135), but poor specificity for tracheal placement. The device may suggest esophageal placement when the tube is in the trachea in patients who are morbidly obese, in late pregnancy, and with pulmonary edema or severe airway obstructive disease (e.g., asthma). These false-positive events occur because either the trachea collapses (obesity and late pregnancy) or air is not easily recruitable from the lung (pulmonary edema and severe airway obstruction). Sensitivity and specificity of EDDs are poor in children younger than 1 year old, and they are not recommended in children weighing less than 20 kg (136).
Advanced Airway Adjuncts
Multiple airway adjuncts are available in cases of failed endotracheal intubation and difficult bag-mask ventilation. Two of these devices, the laryngeal mask airway and esophageal tracheal Combitube, are widely used and discussed in depth in Chapter 38 (Airway Management). These adjuncts are “rescue airways,” a bridge rather than alternate to endotracheal intubation that is readily mastered with appropriate training. Although they facilitate effective ventilation, they do not allow tracheal suctioning or provide reliable airway protection.
Electrical Therapy
Electrical therapy is one of the mainstays of ALS, especially in adults. Electrical energy is used to treat life-threatening cardiac dysrhythmias, which constitutes 16% to 85% (137,138,139,140) of out-of-hospital and 14% to 56% (17,141,142,143,144) of in-hospital cardiac arrests. Recent data suggest that ventricular fibrillation and ventricular tachycardia are decreasing, with only 24% of the initial rhythms in over 36,000 adult arrests being VF- or VT-based on a recent analysis from the National Registry for Cardiopulmonary Resuscitation (NRCPR) (4). In hospitalized children with cardiac arrest, VF is the initial rhythm in approximately 10% of cases and subsequently occurs during 15% of the cases (26). Despite the fall in prevalence, early recognition of a shockable rhythm is critical since the outcome following effective treatment is much better than after asystole or PEA (4). Several different modes of electrical therapies are available for treatment of different rhythm problems. These include defibrillation, cardioversion, and cardiac pacing.
Defibrillation
Defibrillation is defined as delivery of electrical energy resulting in termination of VF for at least 5 seconds following the shock (145,146). The goal is to quickly depolarize the whole myocardium, terminating the rhythm and hoping that a sinus rhythm will start. Defibrillation should not be confused with ROSC or survival. In most adults, the initial postshock rhythm is asystole or an organized slow rhythm without a pulse (i.e., PEA). This observation is the basis for the current guideline recommendation to immediately begin chest compressions after shock delivery.
Defibrillator device
There are two types of defibrillator devices available: (a) manual defibrillator devices require the rescuer to analyze the rhythm and then manually set and determine the electrical energy dose; (b) automatic defibrillator devices analyze the rhythm, determine if a shock is required, and deliver the shock if needed automatically. There are two types of automatic defibrillators: internal implantable cardioverter defibrillator (ICD) and automated external defibrillator (AED). Defibrillators are also characterized by the mode and waveform of electrical current delivered into monophasic and biphasic defibrillators. Animal and human data show that biphasic defibrillators have a higher first shock success in terminating VF compared with monophasic devices; the latter are no longer produced. Manufacturers use various methods of delivering the biphasic energy, and more recently, triphasic and quadriphasic defibrillators are being developed and appear to be potentially more effective than biphasic defibrillators (147,148).
Monophasic defibrillators deliver current in one direction or polarity so current flows from one paddle (or electrode) to the other throughout the duration of shock. As noted, these defibrillators are being replaced by biphasic defibrillators.
Biphasic defibrillators deliver current sequentially in both directions or polarity during one shock. In the first phase, the current moves from one paddle to the other as with monophasic defibrillators, and during the second phase, the current flow reverses direction. Biphasic defibrillators can also be further classified based on the waveform changes into (a) biphasic truncated exponential waveform and (b) rectilinear biphasic waveform. Several randomized trials (149,150,151) showed that defibrillation with biphasic waveforms of relatively low energy (200 J) is safe and has equivalent or higher efficacy for termination of VF than monophasic waveform shocks of equivalent or higher energy, which decreases the risk of myocardial injury and increases shock efficacy.
Defibrillation dose
The optimal energy dose for the first of subsequent shocks required for effective defibrillation remains unknown despite multiple studies (151,152). The ideal shock dose for a biphasic device is one that falls within the range documented as effective using that specific device. It is reasonable to use selected energies of 150 J to 200 J with a biphasic truncated exponential waveform or 120 J with a rectilinear biphasic waveform for the initial shock. For second and subsequent biphasic shocks, the same or higher energy can be given. The rescuer should have knowledge of the type of defibrillator being used and select the energy dose accordingly. Most manual defibrillators are set to an initial default of 200 J of energy. This is not necessarily the optimal dose in all cases, but was selected because it falls within the reported range of doses effective for first and subsequent biphasic shocks. If only a monophasic defibrillator is available, then an energy dose of 360 J is recommended for all shocks.
During shock, the average current delivered is the key determinant of successful defibrillation (153,154,155). Current delivery is determined by the energy level selected and by the patient's transthoracic impedance. The average adult human transthoracic impedance is 70 to 80 Ω (156,157,158). While mean current determines the success of defibrillation, high peak currents during the shock are associated with myocardial injury. Biphasic waveforms deliver lower peak current values compared to monophasic waveforms. If transthoracic impedance is high, a low-energy shock will not generate sufficient current to achieve defibrillation. To improve current delivery, conductive gels are recommended in place of manual paddles. Adhesive pads have the added advantage of reducing the risk of inadvertent rescuer shock. Regardless of the device used, the rescuer needs to press the paddles or pads firmly on the chest wall to ensure a good electrical contact.
The optimal dose for effective defibrillation in infants and children is not known. The upper limit for safe defibrillation is also not known, but doses more than 4 J/kg (as high as 9 J/kg) have effectively defibrillated children (159,160) and pediatric animal models (161) with no significant reported adverse effects. Recommended manual defibrillation (monophasic or biphasic) doses for children are 2 J/kg for the first attempt and 4 J/kg for subsequent attempts.
Electrode position
Either handheld paddles or self-adhesive pads are used for shocks. Electrodes are applied to the bare chest in the conventional sternal-apical (anterolateral) position. The right (sternal) chest pad is placed on the victim's right superior-anterior (infraclavicular) chest and the apical (left) pad is placed on the victim's inferior-lateral left chest, lateral to the left breast. Other acceptable pad positions are placement on the lateral chest wall on the right and left sides (biaxillary) or the left pad in the standard apical position and the other pad on the right or left upper back (avoiding the scapular bone). Similar positions are recommended for children, particularly the anterior-posterior position since many defibrillators have only a single size electrode pad and there should be at least 1 inch between the pads. The rescuer should make sure that electrodes are not overlapping and are not on top of implanted devices or transdermal medicine patches if present. If the patient is wet, the chest should be wiped dry before placement. Another caution is to avoid placing the oxygen source near the electrodes, particularly in children where the distance from the face to the chest is short.
Electrode size
In general, the largest pad or paddle that can be placed on the chest while avoiding contact between the pads or paddles should be used. There should be at least 1 inch between the pads. Paddles that are too small increase the risk of skin burn injury.
Automatic rhythm analysis and automatic external defibrillators
AEDs are computerized compact devices that use voice and visual prompts to guide lay rescuers and health care providers to safely defibrillate VF or pulseless VT (139,162,163,164). In a large prospective randomized trial (165) funded by the AHA, the National Heart, Lung, and Blood Institute (NHLBI), and several AED manufacturers, lay rescuer CPR AED programs in targeted public settings doubled the number of survivors from out-of-hospital VF SCA when compared with programs that provided early EMS call and early CPR.
Despite limited evidence, AEDs should be considered within the hospital as a way to facilitate early defibrillation (a goal of <3 minutes from collapse), especially in areas where staff have limited to no rhythm recognition skills or defibrillators are used infrequently.
For children 1 to 8 years of age, the rescuer should use a pediatric dose-attenuator system with the AED if one is available (160). If the rescuer provides CPR to a child in cardiac arrest and does not have an AED with a pediatric attenuator system, the rescuer should use a standard AED.
Electrical Cardioversion
Electrical cardioversion is used for some life-threatening arrhythmias causing rapid cardiovascular deterioration. These include VT and supraventricular tachycardias (SVTs), such as paroxysmal atrial tachycardia (PAT), atrial flutter, or atrial fibrillation with a rapid ventricular response. The electrode size and positioning is the same as that used in defibrillation; the difference between cardioversion and defibrillation is described below.
Technique
Unlike defibrillation, cardioversion must be synchronized with the patient's electrocardiogram (ECG). The ideal discharge point is during the upstroke of the R wave of the QRS complex. Delivery of the energy during the T wave of the QRS may result in ventricular fibrillation. Most commercially available defibrillators automatically coordinate the discharge to the patient's ECG if the machine is placed in the synchronized mode and the QRS complex is of adequate size for consistent detection. If the defibrillator does not “sense” the QRS complex, increasing the ECG gain improves sensing. Cardioversion should never be attempted with quick-look paddles, because ECG artifact may make synchronization impossible. Unsynchronized cardioversion should only be used when the available equipment does not allow synchronization.
Energy level
The amount of energy recommended for emergency cardioversion varies with the rhythm (166,167); 100 J is recommended for atrial fibrillation and 50 J for atrial flutter (168). Monomorphic ventricular tachycardia responds well to cardioversion, and 100 J should be attempted first. Pulseless ventricular tachycardia behaves like ventricular fibrillation, and 200 J should be used initially. For cardioversion in conscious patients, sedation with intravenous diazepam, midazolam, or methohexital is indicated, and the cardioversion accomplished with the lowest energy possible (50–200 J). In children, the recommended initial cardioversion dose is 0.5 to 1 J/kg.
External Cardiac Pacing
While, in general, external (transcutaneous) pacing is not recommended for patients in asystolic cardiac arrest, it is our opinion that it should be always considered in the ICU or other critical care areas of the hospital where the device and adequate skill are promptly available. However, three randomized controlled trials (169,170) of fair quality indicated no improvement in the rate of admission to hospital or survival to hospital discharge when paramedics or physicians attempted to provide pacing in asystolic patients in the prehospital or hospital (emergency department) setting. Pacing can be considered in patients with symptomatic bradycardia when a pulse is present.
Pharmacologic Therapy
Pharmacologic therapy in CA is used to increase the rate of ROSC and terminate or limit the risk of recurrent arrhythmias. It is recognized that there are no placebo-controlled studies showing that any vasopressor during human CA increases survival to discharge; indeed, some studies questioned the benefit of their use (171). For obvious reasons, it is unlikely that a large prospective randomized study on this issue will ever be available. However, drug administration is now a secondary priority during CPR with primary emphasis placed on high-quality chest compressions with minimal hands-off time. Since there is little evidence for their use, the number of pharmacologic agents recommended during CPR decreased.
Route of Administration for Resuscitation Medications
It is important to remember that a central venous line may not be available at the time of the arrest, nor is its immediate placement necessary to ensure survival. Peripheral intravenous access can be used effectively with the advantage of not interrupting CPR. When only a peripheral vascular access is available, it is crucial to rapidly follow the medication bolus with a 10- to 20-mL fluid bolus to ensure central delivery. If obtaining any venous access is difficult despite numerous attempts, intraosseous (IO) cannulation is an effective alternate for drug delivery. Studies in both children (172,173) and adults (174) suggest the effectiveness of this route in all age groups. Commercially available kits are available for easy use.
If IV or IO access cannot be achieved, then some resuscitation medications can be administered via instillation through an ET, if available. Lipid-soluble medications that can be delivered via ET are lidocaine, epinephrine, atropine, naloxone, and vasopressin. This route, however, results in much lower blood concentrations compared with IV administration. Optimal doses of the medications delivered via the ET route are not known, but it is recommended to administer at least 2 to 2½ times the IV recommended doses. In fact, animal data suggest that using standard intravenous epinephrine doses via the ET route may not achieve high enough plasma concentrations to be effective (175,176).
Once vascular access is achieved, resuscitation drugs should be immediately readministered if cardiac arrest is still present.
Epinephrine
Epinephrine is the most commonly used medication during CPR. Epinephrine's primary action in CA is to increase the coronary perfusion pressure through systemic vasoconstriction mediated by its α-adrenergic effects. The β-adrenergic effects are relatively unimportant. Indeed, even when complete β-adrenergic blockade is used in an animal cardiac arrest model, epinephrine is effective, whereas α-adrenergic blockade completely eliminates epinephrine's effects (177).
Epinephrine is used primarily during CA due to asystole and PEA. It is a second-line agent used for shock-refractory VF or pulseless VT. Although there are no clinical trials demonstrating that epinephrine is effective in CA, there is substantial animal data and anecdotal clinical experience that epinephrine elevates the coronary perfusion pressure and thus myocardial blood flow. There are little pharmacologic data supporting the currently recommended dose of 1 mg of epinephrine in adult cardiac arrest and 0.01 mg/kg in children. Epinephrine should be given intravascularly whenever possible since intratracheal doses are erratically absorbed as noted above. If only the endotracheal route is available, the dose should be increased to 2 to 2.5 mg in adults and 0.1 mg/kg in children.
Since epinephrine's beneficial effect is through systemic vasoconstriction, it seems reasonable to speculate that higher doses would produce a greater increase in coronary and cerebral perfusion pressure. This hypothesis was supported by initial animal data (178), but subsequent animal studies (179,180) and clinical trials in adults (181,182) and children (183) failed to show a beneficial effect. Indeed, clinical experience suggests that high-dose epinephrine is harmful rather than beneficial and is only indicated in clinical conditions characterized by poor adrenergic responsiveness, such as severe septic shock and β blocker, neuraxial anesthesia, or systemic bupivacaine overdose.
Vasopressin
Vasopressin is an endogenous antidiuretic hormone that, when given at high doses, causes vasoconstriction by directly stimulating vascular smooth muscle V1 receptors (184). Vasopressin improves coronary perfusion pressure, but unlike epinephrine, offers theoretical advantages of cerebral vasodilation, possibly improving cerebral perfusion. Its lack of β1-adrenergic activity potentially avoids unnecessary increases of myocardial oxygen consumption, resulting in postresuscitation arrhythmias. Vasopressin has a longer half-life of 10 to 20 minutes compared to the 3 to 5 minutes observed with epinephrine.
Several human studies suggested that vasopressin achieved a comparable ROSC in CA, although no additional benefit was seen compared with epinephrine (185,186). A recent meta-analysis showed a trend favoring vasopressin (187) compared to epinephrine. Recent guidelines continue to recommend epinephrine as the agent of choice, but one dose of vasopressin 40 units IV/IO is now indicated as an alternative to replace the first or second dose of epinephrine in all CA including asystole and PEA.
Vasopressin is not currently recommended for pediatric use since in an animal model of pediatric asphyxial CA, ROSC was higher in the epinephrine group (188). Vasopressin is contraindicated in conscious patients with ischemic heart disease as it may provoke angina. Other adverse effects include increased mesenteric and renal vascular resistance, bronchial constriction, and uterine contractions in women.
Sodium bicarbonate
Metabolic and respiratory acidosis develops during CA resulting from anaerobic metabolism, leading to lactic acid generation and inadequate ventilation along with reduced blood flow during CPR, which leads to inadequate pulmonary delivery of carbon dioxide for elimination. Untreated acidosis suppresses spontaneous cardiac activity, decreases the electrical threshold required for the onset of ventricular fibrillation, decreases ventricular contractile force, and decreases cardiac responsiveness to catecholamine such as epinephrine. An elevated PCO2 tension probably is more detrimental to myocardial function and catecholamine responsiveness than metabolic acidosis. CO2 readily diffuses across myocardial cell membranes, causing intracellular acidosis and resulting in life-threatening derangements of myocardial function. Likewise, cerebrospinal fluid acidosis may occur secondary to the diffusion of CO2 across the blood–brain barrier, producing postarrest cerebral acidosis. Since sodium bicarbonate buffering of excess protons transiently increases the PCO2 tension, sodium bicarbonate administration without sufficient ventilation and circulation to remove the CO2 that it produces seems to be more detrimental than helpful (189,190). Sodium bicarbonate therapy may be useful after interventions such as defibrillation, cardiac compression, intubation, ventilation, and more than one trial of epinephrine have been used. Some evidence suggests that any benefit from bicarbonate therapy may be related more to volume expansion from its high sodium content rather than its buffering effects (191).
If arterial blood gas and pH measurements are not available, the recommended initial dose of sodium bicarbonate is 1 mEq/kg intravenously; half of this dose may be repeated at 10-minute intervals. For pediatric patients, the 1 mEq/kg dose should be diluted 1:1 with sterile water to reduce the osmolality.
Administration of excessive amounts of sodium bicarbonate can result in metabolic alkalosis, leftward shift of the oxyhemoglobin dissociation curve, interference with tissue oxygenation, hypernatremia, hypokalemia, and worsening of respiratory and myocardial acidosis if adequate ventilation and perfusion cannot be achieved and maintained.
Atropine
Atropine is used during CPR for its vagolytic actions. A reduced vagal influence on the heart improves both the rate of sinoatrial node discharge and impulse conduction through the atrioventricular (AV) conduction system, with a resulting increase in heart rate.
Atropine is used in sinus bradycardia when accompanied by hypotension or frequent premature ventricular contractions (PVCs) secondary to unsuppressed ectopic electrical activity arising in the area of injured tissue during the prolonged period after repolarization. Sinus bradycardia after myocardial infarction may predispose the heart to the onset of ventricular fibrillation (192). When profound bradycardia is present, acceleration of the heart rate above 60 beats per minute (bpm) may improve cardiac output and reduce the incidence of ventricular fibrillation. Atropine also may be useful for treating high-degree AV block with a slow ventricular rate and asystole occurring after increased parasympathetic tone that results in suppression of the electrical activity to the heart (193).
The dosage of atropine for severe symptomatic bradycardia is 0.5 to 1.0 mg intravenously repeated every 3 to 5 minutes until the desired pulse rate is obtained or a maximum of 0.04 mg/kg has been given. A larger dose has little therapeutic value, and a smaller dose may actually slow the heart rate. Endotracheal dose is 2 to 2.5 mg. Although not routinely recommended in the treatment of asystole, when used, incremental doses of 1 mg are preferred, using up to three doses given every 3 to 5 minutes of CA.
Ventricular tachycardia and fibrillation after intravenous administration of atropine have been reported. In second-degree type II heart block, a paradoxical decrease in ventricular response may result (189).
Lidocaine
Lidocaine decreases ectopic electrical myocardial activity by raising the electrical stimulation threshold of the ventricle during diastole. In ischemic myocardial tissue after infarction, it may suppress re-entrant arrhythmias such as ventricular tachycardia or fibrillation. There is now good evidence, however, that other agents are superior to lidocaine in terminating VT (194,195); hence, it is not considered a first-line agent. The 2005 guidelines recommend lidocaine only when amiodarone is not available.
Lidocaine may be used in stable monomorphic VT and polymorphic VT with normal or prolonged QT interval if ventricular function is not decreased.
The loading dose of lidocaine is approximately 1 to 1.5 mg/kg given as an intravenous bolus. If needed, repeat 0.5 to 0.75 mg/kg every 5 to 10 minutes, up to a total of 3 mg/kg, followed by a continuous infusion of 30 to 50 µg/kg/minute (1–4 mg/minute in a 70-kg patient) (192).
Excessive doses may induce heart block or depression of sinus node discharge, especially in patients with pre-existing conduction disturbances. Toxicity may occur in oliguric or anuric patients because renally excreted lidocaine degradation products also have pharmacologic effects and toxic potential. Early signs of lidocaine toxicity are due to central nervous system (CNS) effects and include anxiety, loquacity, tremors, metallic taste, and tinnitus. These may be followed by somnolence, respiratory depression, apnea, and, in severe cases, cardiovascular collapse. If CNS irritability occurs, lidocaine therapy should be withdrawn and a barbiturate or a benzodiazepine may be administered if deemed necessary and if the patient's circulatory status is sufficiently stabilized.
Procainamide
Procainamide suppresses both atrial and ventricular arrhythmias with similar mechanisms of action to those of lidocaine. It may suppress an ectopic irritable focus and blocks re-entrant arrhythmias by slowing electrical conduction. Procainamide may be superior to lidocaine in terminating VT (196).
Procainamide is used in the management of PVCs, ventricular tachycardia, and persistent ventricular fibrillation, but amiodarone is usually preferred.
Incremental bolus injections of procainamide are slowly infused at 20 mg/minute until (a) the arrhythmia is controlled, (b) hypotension occurs, (c) the QRS complex is widened 50% from baseline, or (d) a total dose of 17 mg/kg (1.2 g in a 70-kg adult) is given followed by a continuous infusion of 1 to 4 mg/minute to prevent recurrent arrhythmias. Other effective administration schedules have been tested and approved; all are designed to maintain a therapeutic plasma level of 4 to 8 µg/mL.
Procainamide can have profound myocardial depressant effects, especially after myocardial infarction; therefore, continuous ECG and arterial blood pressure monitoring are mandatory. End points of therapy include hypotension and a greater than 50% widening of the QRS complex.
Amiodarone
IV amiodarone is a complex drug with effects on sodium, potassium, and calcium channels on myocardial cells as well as α- and β-adrenergic blocking properties. The 2005 guidelines denote that it is the preferred agent for both atrial and ventricular arrhythmias, especially in the presence of impaired cardiac function.
Amiodarone is recommended for narrow-complex tachycardias that originate from a re-entry mechanism (re-entry SVT); ectopic atrial focus; control of hemodynamically stable VT, polymorphic VT with a normal QT interval, or wide-complex tachycardia of uncertain origin (195,197); and control of rapid ventricular rate due to accessory pathway conduction in pre-excited atrial arrhythmias with AV nodal blockade in patients with preserved or impaired ventricular function (198).
In the treatment of arrhythmias with a pulse, 150 mg amiodarone is given IV over 10 minutes, followed by a 1 mg/minute infusion for 6 hours and then a 0.5 mg/minute maintenance infusion over 18 hours. Supplementary infusions of 150 mg can be repeated every 10 minutes as necessary for recurrent or resistant arrhythmias to a maximum manufacturer-recommended total daily IV dose of 2.2 g. One study found amiodarone to be effective in patients with atrial fibrillation when administered at relatively high doses of 125 mg/hour for 24 hours (total dose 3 g) (199).
When used in the treatment of VF or pulseless VT, a bolus dose of 300 mg is recommended diluted in 20 to 30 mL of D5W. A single second dose may be given (150 mg) in 3 to 5 minutes for shock-refractory VF or VT. In children, 5 mg/kg is given as a rapid bolus and may be repeated up to 15 mg/kg.
The major adverse effects of amiodarone are hypotension and bradycardia, which can be prevented by slowing the rate of drug infusion. In addition, amiodarone can increase the QT interval, and therefore its use should be carefully considered when other drugs that can prolong the QT interval are administered.
Calcium
Calcium ion plays a critical role in myocardial contractility and action potential generation, but studies have shown no benefit of calcium in CA (200,201), and therefore calcium probably should not be considered during CA only when acute hyperkalemia or hypocalcemia is suspected or calcium channel blockers were administered. The use of calcium during CA is controversial because of the fear that it may produce a tetanic contraction of an irritable myocardium or depression of the sinus node, resulting in asystole. Since maintenance of the 10,000-fold higher extracellular calcium concentration compared with the intracellular concentration is energy dependent, exposing hypoxic-ischemic cells to high plasma calcium concentrations may result in calcium overload, which activates a number of toxic mechanisms. This effect is particularly worrisome in the brain because it is so sensitive to hypoxia.
When indicated, the recommended dose is 5 to 10 mL of a 10% solution of calcium chloride (8–16 mg/kg). A bolus may be repeated at 10-minute intervals, if necessary. Calcium salts cannot be mixed directly with sodium bicarbonate because it precipitates as calcium carbonate. Several calcium preparations are available for intravenous use: Calcium chloride and calcium gluconate are the most popular. Calcium gluconate is given in a dose of 6 to 8 mL if peripheral IV access is available. Undiluted calcium chloride given through a peripheral vein may cause sclerosis and tissue injury; therefore, if a central site is not available and the patient is not in cardiac arrest, it should either be diluted or calcium administered in a less irritating form (e.g., calcium gluconate). In children, a dose of 10 to 20 mg/kg of calcium chloride is recommended.
Rapid administration of a large bolus of calcium chloride, especially through a central venous catheter, may produce severe sinus bradycardia or sinus arrest. Calcium must also be used cautiously in patients receiving digitalis, because it can produce or accentuate digitalis toxicity.
Magnesium
Magnesium is recommended for the treatment of torsades de pointes VT with or without cardiac arrest. It has not been shown to be helpful during non–torsades de pointes VT (202,203). Although magnesium is a calcium channel blocker and theoretically may protect ischemic cells from overload, there are no data supporting its routine use in cardiac arrest. If needed, magnesium is given at a dose of 1 to 2 g diluted in D5W over 10 to 60 minutes. In children, a dose of 25 to 50 mg/kg is used.
Rapid administration may result in hypotension and bradycardia. Magnesium also should be used cautiously in patients with renal failure.
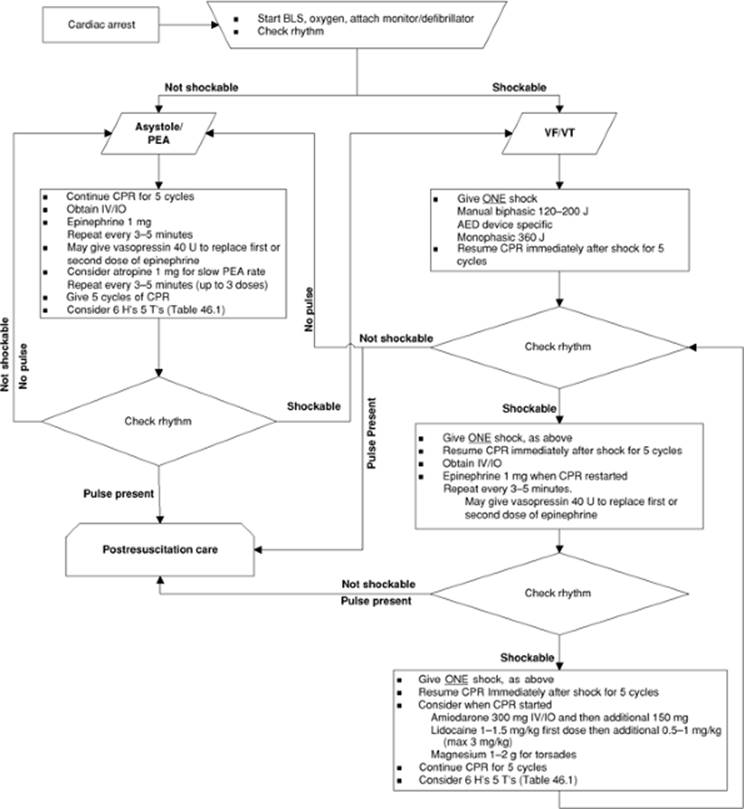
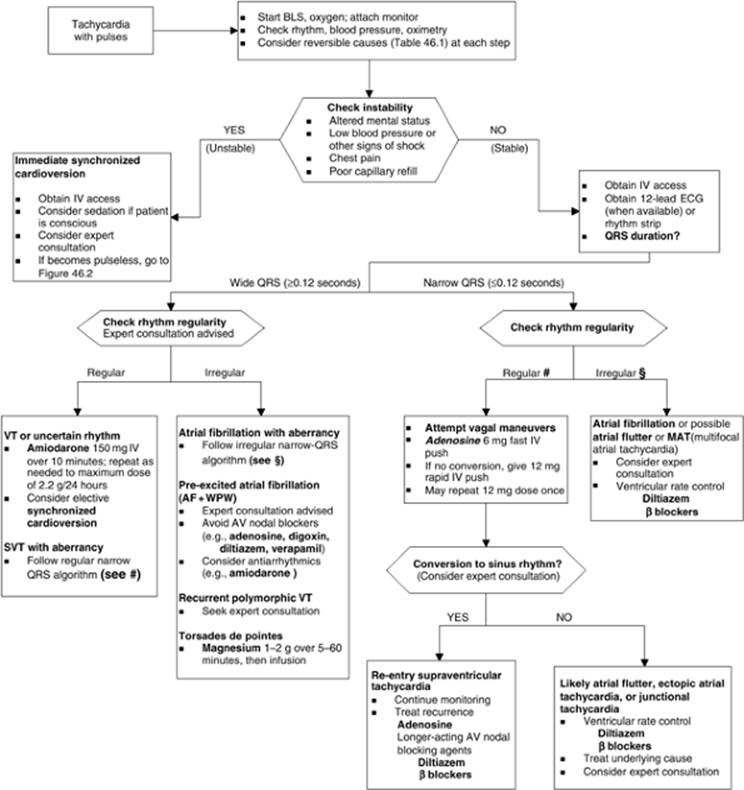
Algorithms for Advanced Life Support
The treatment algorithms of pulseless cardiac arrest and tachycardia with pulse are summarized in Figures 46.2 and 46.3, respectively.
Monitoring during Cardiopulmonary Resuscitation
Clinical
There are no reliable clinical indicators of the effectiveness of CPR provided. Although feeling for a pulse during chest compressions is used clinically to assess the effectiveness of chest compressions, no study has validated this technique. Moreover, data show that a palpated femoral pulse may be from retrograde venous pulsation rather than antegrade arterial flow (204).
Hemodynamics
When invasive arterial and central venous pressure monitoring are present, coronary perfusion pressure (CoPP) monitoring is possible. It is calculated as CoPP = aortic diastolic pressure minus the right atrial pressure (CoPP = DBP – RAP). A CoPP >15 mm Hg is predictive of ROSC (193,205) and increased CoPP correlates with improved 24-hour survival in animal studies (206).
Arterial Blood Gas
The acidosis gradient between arterial and central venous blood (largely determined by PCO2) reflects the effectiveness of blood flow during low-flow states such as CPR (207). Similarly, animal studies and case reports report similar arteriovenous differences in PCO2 between arterial and venous blood at the organ level (e.g., heart) and the entire organism (208,209,210). These studies suggest that measurement and comparison of a venous and arterial blood gas may be predictive during cardiac arrest. Furthermore, it suggests that the arterial blood gas does not accurately reflect the severity of tissue acidosis, hypoxia, or hypercarbia during both in-hospital and out-of-hospital cardiac arrest. Instead, the arterial blood gas often reflects the effectiveness of ventilation during cardiac arrest. Similarly, both animal and human data show a significant worsening of the arterial blood gas values for acidosis and oxygenation with ROSC, representing the washout of built-up tissue acids.
End-tidal Carbon Dioxide
Aerobic and anaerobic cellular metabolism generates CO2, which rapidly diffuses out of the cell and into tissue capillaries, is transported to the lungs, is exhaled, and can be measured as end-tidal CO2(211,212). Under normal conditions, end-tidal PCO2 is 2 to 5 mm Hg less than the PaCO2. Although ischemic hypoxia can alter the respiratory quotient, systemic metabolism changes little during CPR, which is relatively brief, so that changes in end-tidal PCO2 during CPR typically reflects changes in the effective pulmonary blood flow (211,212). Under conditions of constant minute ventilation, end-tidal CO2 is linearly related to cardiac output, even during extremely low blood flow rates (213), and is therefore useful clinically as a monitor of perfusion during shock and CPR. Indeed, a number of studies showed that end-tidal CO2 varies directly with cardiac output during cardiac arrest (214,215,216) and provides a useful indicator of the efficacy of resuscitation efforts. Not surprisingly, ETCO2 also predicts outcome in adults (217,218,219,220) and children (221). Additionally, capnography is used in resuscitation research as an indication of pulmonary blood flow, which serves as a proxy for the direct measurement of cardiac output (120,222,223).
Following the administration of epinephrine, end-tidal CO2 typically falls, suggesting that the relationship of end-tidal CO2 to cardiac output is altered, but in fact it is maintained and reflects a global fall in cardiac output due to changes in pulmonary and peripheral vascular resistance and preferential redirection of blood flow (219). When used in cardiac arrest, epinephrine decreases pulmonary blood flow (i.e., overall cardiac output) and end-tidal CO2 while increasing coronary perfusion pressure and myocardial blood flow because of increased peripheral vascular resistance (224).
Coronary artery perfusion pressure also correlates closely with end-tidal CO2 (218,225). Several studies of end-tidal carbon dioxide during low blood flow states found that levels changed significantly with changes in minute ventilation (226). When minute ventilation doubled, end-tidal carbon dioxide decreased by 50%, and when minute ventilation decreased by 50%, end-tidal carbon dioxide doubled. Thus, end-tidal carbon dioxide varies inversely with minute ventilation and can be used to monitor ventilation during low-flow conditions. If both perfusion and ventilation are changed, end-tidal carbon dioxide levels can be difficult to interpret.
Postresuscitation Care
After ROSC, the risk of mortality remains high for cardiac arrest patients as most deaths happen during the first 24 hours following successful resuscitation (227,228). Postresuscitation care is one of the most important elements of CPR that can potentially result in improved outcome (229). The goals of postresuscitation care are to (a) optimize cardiovascular and neurologic support, (b) identify the possible cause of arrest and prevent recurrence, and (c) use measures that may improve long-term neurologic outcome.
|
|
|
Figure 46.2. Suggested treatment algorithm for pulseless cardiac arrest. It is important that resuscitation drugs should be given during the cardiopulmonary resuscitation (CPR) cycles to minimize “no CPR” time. BLS, basic life support; PEA, pulseless electrical activity; VF, ventricular fibrillation; VT, ventricular tachycardia; AED, automated external defibrillator; IO, intraosseous. (Adapted and modified from 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2005;112[24]SIV-1–IV-211.) |
After ROSC, vital signs, clinical and laboratory signs of tissue perfusion, the occurrence of cardiac arrhythmias, and neurologic status should be frequently monitored. Obtain appropriate intravenous and intra-arterial vascular access as needed to monitor the patient and obtain frequent laboratory studies. Obtain an arterial or central venous blood gas (preferably both) to assess for the presence of acid-base abnormalities, and obtain electrolytes including magnesium, phosphorus, ionized calcium, and blood urea nitrogen (BUN) to ensure that there are no electrolyte abnormalities and to help assess renal function. The gradient between arterial and venous oxygen saturation can help evaluate the adequacy of tissue perfusion. Trained personnel with resuscitation equipment must accompany the patient during transport to an appropriate monitoring unit.
|
|
|
Figure 46.3. Suggested treatment algorithm for tachycardia with pulse. BLS, basic life support; ECG, electrocardiogram; VT, ventricular tachycardia; SVT, supraventricular tachycardia; WPW, Wolff-Parkinson-White syndrome. (Adapted and modified from 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2005;112[24]SIV-1–IV-211.) |
It is increasingly recognized that postresuscitation care has an important effect on ultimate survival following cardiac arrest. Studies are currently evaluating optimal treatments for postresuscitation care (230). The following are generally accepted as part of postresuscitation care.
Glucose Control
Many studies showed a strong association between hyperglycemia after cardiac arrest and poor neurologic outcome (28,231,232,233). Hyperglycemia developing after cardiac arrest likely reflects the effects of epinephrine and endogenous stress hormones as well as reduced glucose metabolism by the injured brain. What is not clear, however, is whether control of the glucose concentration following cardiac arrest results in an improved outcome. Data from studies in adult surgical and medical critical care patients showed reduced mortality with tight glucose control (234,235). Based on these data in critically ill patients, it seems reasonable to normalize the glucose concentration in patients after cardiac arrest, but the evidence for this approach is lacking. Furthermore, it is not clear if glucose should be restricted or if insulin should be used to normalize the glucose concentration, but the general approach is to frequently monitor the glucose concentration and use an insulin infusion to normalize the glucose concentration if it is elevated. The target range for glucose concentration in this situation is not known, but a range of 80 to 110 mg/dL is commonly used. The risk of this approach is that hypoglycemia may occur, resulting in further injury to at-risk brain cells.
Respiratory System
Some respiratory dysfunction can be present after ROSC, and patients require ongoing mechanical ventilation and oxygen administration. ET position should be assessed upon arrival to the critical care unit. Ventilator support should be adjusted to help normalize the patient's acid-base status and work of breathing, while recognizing that high respiratory rates and airway pressure may impair venous return and thus cardiac output. If an end-tidal CO2 monitor is available, ventilation rate should be adjusted to maintain end-tidal CO2 within a range of about 35 mm Hg to 45 mm Hg. In patients with obstructive pulmonary disease and increased resistance to exhalation, a lower ventilation rate should be used (e.g., six to eight breaths per minute) to prevent air trapping and to allow enough time for complete exhalation (132).
If more severe injury is present, it is usually due to pulmonary edema, gastric content aspiration, or acute respiratory distress syndrome (ARDS). While generally in these cases oxygenation may be improved by the application of positive end-expiratory pressure, more detailed treatment guidelines are reviewed in other sections of this textbook.
Cardiovascular System
Cardiac function and rhythm can be altered after cardiac arrest. This results from both global ischemia and reperfusion injury post ROSC or by the effect of defibrillation itself, which can cause myocardial stunning (236,237). Hemodynamic instability is common after cardiac arrest and may be multifactorial including a combination of cardiac dysfunction, altered capillary permeability, variations in venous and arterial vascular tone, and the elaboration of cytokines that may mimic sepsis (238). Invasive hemodynamic monitoring and judicious use of inotropes with vasopressor or vasodilators properties may be needed (227).
Although post–cardiac arrest arrhythmias may be detrimental, prophylactic treatment may also produce adverse effects, so prophylactic antiarrhythmics are not recommended. If an antiarrhythmic was used to achieve ROSC, then it should be continued, although the selection of antiarrhythmic agents for longer-term use is best made in consultation with a cardiologist.
Central Nervous System
After ROSC, the brain often experiences an initial brief increased blood flow (“hyperemia”) phase, which is followed by a significantly reduced (“no-reflow phenomenon”) phase due to microvascular dysfunction and thrombosis (239,240). In addition, excitatory neurotransmitters are released, increasing metabolic demand in vulnerable areas of the brain such as the hippocampus. In general, efforts are focused on optimizing cerebral perfusion pressure by treating hypotension and maintaining, when feasible, a 20% to 30% higher than normal mean arterial pressure, especially in cases at risk for increased intracranial pressure. Fever and seizures can be seriously detrimental to the brain and should be aggressively treated. There are insufficient data to recommend for or against the use of prophylactic anticonvulsants in postcardiac arrest.
Temperature Control
Avoiding Hyperthermia
Temperature dysregulation may be present after ROSC, which may result from brain injury as shown in animal models of cardiac arrest (241,242,243,244). Fever is associated with worse neurologic outcome in humans after cardiac arrest or ischemic brain injury (245,246). Antipyretics and surface cooling techniques should be used to achieve normothermia. Some experts recommend routine administration of antipyretics, and the 2005 guidelines recommend frequent or continuous temperature monitoring and aggressive treatment of fever in the postarrest setting.
Hypothermia after Cardiac Arrest
In 2002, two prospective randomized controlled clinical trials of therapeutic hypothermia were conducted in comatose survivors after cardiac arrest in adults. In the Australian study (247), survivors of out-of-hospital VF cardiac arrest with coma were randomized in the field by EMS providers to hypothermia or normothermia, with cooling beginning in the prehospital setting. Cooling was maintained for 12 hours followed by passive rewarming. Good outcome (survival and good functional recovery) was observed in 21 of 43 (49%) hypothermic patients versus 9 of 34 (26%) normothermic patients (p = 0.046; number needed to treat [NNT] = 5; 95% confidence interval [CI], 2.3–81). A larger European trial in a similar patient population (248) showed favorable neurologic outcome at 6 months with the use of 24 hours of therapeutic hypothermia begun after hospital arrival following out-of-hospital ventricular fibrillation cardiac arrest (75 of 136 [55%]) compared with the normothermic group (54 of 137 [39%]). The risk ratio for this study was 1.40 (95% CI, 1.08–1.81) and the NNT was 7 (95% CI, 3.6–25). Subsequently, the ILCOR recommended the use of therapeutic hypothermia for adult patients who were comatose following ventricular fibrillation cardiac arrest and suggested that hypothermia should be considered in comatose patients with other rhythms after out-of-hospital cardiac arrest (249).
Several neonatal trials also showed a beneficial effect of 72 hours of therapeutic hypothermia following perinatal asphyxia (250,251), but there are no clinical data in children to recommend for or against the routine use of hypothermia in the postarrest setting.
Hypothermia can be applied in two ways after cardiac arrest: (a) permissive hypothermia, maintaining the mild hypothermia >33°C that is often present in postarrest patients; or (b) induced hypothermia, where patients are actively cooled to the 32°C to 34°C range. Currently, consensus guidelines for induction, maintenance, and weaning of therapeutic hypothermia do not exist. Some recent studies have explored methods of internal cooling using cold saline boluses or endovascular catheters (252). We recently surveyed a sample from the pediatric critical care community and found that despite awareness of this technique, it is not widely applied. There is variation in methods, temperature goal, and duration of cooling, with most clinicians using external cooling techniques with target temperature ranging from 33°C to 35°C for 12 to 24 hours (253).
Prolonged or deeper hypothermia increases the risk of infection, coagulopathy, thrombocytopenia, renal impairment, and pancreatitis (254,255). It is likely that induced hypothermia will affect drug metabolism, but there are little objective data to guide clinical therapy. Further studies are needed to develop standard protocols for this brain-protective therapy.
Extracorporeal Life Support and Cardiopulmonary Resuscitation
Rapid use of extracorporeal membrane oxygenation (ECMO) in the context of CPR is termed extracorporeal cardiopulmonary resuscitation (ECPR). This technique is invasive and requires emergent cannulation of a large central vein and artery. Venous blood is passed through a membrane oxygenator for oxygenation and removal of CO2 and returned in an artery to augment blood circulation. The setup and personnel required for this procedure are available in few large tertiary care centers with an in-house multidisciplinary team available to rapidly prepare the ECMO circuit. ECPR has been used in both pediatric and adult patients with primarily cardiac disease with a reported survival of 64% in neonates, 50% in children, and 51% in adults (256,257). In a large single-center report (258), 64 children who failed initial advanced life support were placed on ECMO during active CPR with the median duration of chest compressions of 50 minutes (range 5–105 minutes); remarkably, 33 (50%) survived for 24 hours and 21 (33%) survived to hospital discharge. Five of the survivors were noted to have significant neurologic impairment at hospital discharge. Use of extraordinary measures like ECPR and ECMO seems reasonable if the patient's condition is reversible and ECMO can be established before irreversible brain damage happens during the cardiac arrest. One advantage of extracorporeal circulatory support is that it is relatively easy to rapidly cool the patient and maintain the target temperature for brain protection.
Ethical Considerations
Termination of Cardiopulmonary Resuscitation Efforts
CPR is inappropriate when survival is not expected. Even in the ICU, CPR can be administered by rescuers who may not know the patient or the advanced directive status of the patient. There are few criteria that can reliably predict the futility of CPR. Therefore, it is recommended that all patients with cardiopulmonary arrest receive CPR with the following exceptions:
1. There is a valid Do Not Attempt Resuscitation (DNAR) order, which can be verified.
2. Signs of irreversible death are already present (e.g., rigor mortis, decapitation, decomposition, dependent lividity).
3. No physiologic benefit can be expected with further CPR.
4. In newborns, gestational age or congenital abnormality is related to almost certain early death.
In the ICU, CPR is started without a physician's order, which is based on implied consent for emergency treatment. As a minimal standard, it is expected that all nursing staff in the unit are able to immediately start BLS and be knowledgeable on the use of an automatic external defibrillator. However, the decision to stop CPR should be made by a physician treating the patient, ideally familiar with the patient's pre-existing conditions. Although many factors have been studied as a guide to determine the futility of CPR, such as the presence of comorbidities, time to CPR, time to defibrillate, and initial rhythm, none of these either alone or in combination reliably predicts chances of neurologically intact survival (259,260). On rare occasions, good outcome with prolonged CPR has been reported (261,262,263). It is acceptable to prolong resuscitative efforts in children with recurrent VF or VT, drug toxicity, or a primary hypothermic insult.
Family Presence during Cardiopulmonary Resuscitation
It has been a common practice to exclude family of the arrest victim during CPR efforts. Helping the family of a dying patient is an important part of CPR and should be done in a compassionate manner considering the family's cultural and religious beliefs and practices. Although there is concern that allowing family presence may become disruptive, interfere with resuscitation, cause them to experience syncope, and increase the risk of legal liability (264,265,266), these concerns were not substantiated by good evidence, and in the authors' experience these factors are not a major issue. Family surveys following CPR suggested that the majority of family members want to be present during CPR (267,268). It is also suggested that being present at the time of death was comforting and helped with adjustment later (269). In pediatric arrest, most parents surveyed wanted an option to be present during CPR (270). The resuscitation team should be sensitive to the family's presence and a team member should be assigned to comfort the family, answer questions, and clarify the procedures.
Future Considerations
Current Performance during Cardiopulmonary Resuscitation
Although U.S. and international guidelines continue to recommend high-quality CPR to improve survival from cardiac arrest (271), disturbing evidence seems to indicate that this is not happening in most cases. Studies suggest that bystander CPR in witnessed cardiac arrest is performed in only about one third of the cases (272,273). There are several suggested reasons for this finding: CPR algorithms are complicated, training is inadequate, retention of skills is difficult, and both lay rescuer and professionals are afraid of transmission of diseases (274,275,276).
An out-of hospital cardiac arrest observational study in 176 adults showed that chest compressions were given only half of the available time during the resuscitation event. When CPR was performed by professional rescuers, compression time increased but still averaged 80% of the total resuscitation time (94). In the same setting (277), it was reported that police and firefighters performed CPR correctly only 45% of the time while waiting for ambulance personnel. Prehospital data indicate that most of the time “wasted” without CPR could be explained by programmed interruptions from automated defibrillators or pulse check. The quality of in-hospital CPR is also discouraging. Even highly trained hospital personnel such as ICU physicians often fall short of CPR guidelines during resuscitation efforts (95).
One other issue is the inability to completely relax the chest during the decompression phase (85). Recent laboratory data suggest that rescuer fatigue is an important cause of poor BLS CPR. Reduced performance due to fatigue was noted after just 1 minute and the magnitude was proportional to the compression speed. In a manikin model, an increased compression-to-ventilation ratio of 15:2 provided only 14.5% more compressions than a C:V ratio of 5:1, but nearly 81% of the rescuers perceived that a C:V ratio of 15:2 was more tiring than a 5:1 ratio (104). The quality of compressions seems to decrease significantly after 1 minute and then again between 4 and 5 minutes of CPR, suggesting the need for frequent rescuer rotations, between 1 and 5 minutes, to optimize the effectiveness of chest compression. Interestingly, subjective awareness of fatigue is usually present only after 5 minutes, despite the substantial decrease of chest compression depth at 1 minute (278). Decay of chest compression quality always includes rate and depth.
Studies have shown that the decay of skill mastery is almost immediate after a CPR class with a trend toward too shallow compressions by lay rescuers (279) and too deep compressions by health professionals (280). In general, repeated manikin training is more successful in correcting too shallow compressions than too deep (280).
Another study revealed that most trained personnel provided too much ventilation, ~30 breaths/minute, during out-of-hospital cardiac arrest. Hyperventilation increases mean airway pressure, resulting in decreased venous return and cardiac output, which worsens survival (40).
Training Needs for Quality Improvement
Involvement of Lay Rescuers
Few advanced life support interventions improve survival of SCA patients. It is recognized that early and effective CPR and defibrillation are effective. Therefore, there is a need to increase access to CPR education and improve CPR training quality and retention of skills.
Feedback Devices
Use of devices that can help rescuers by prompting or giving voice feedback or tone may increase the effectiveness of CPR. These devices improve ETCO2 and quality of CPR in both in-hospital and out-of-hospital settings (98,281,282,283).
Medical Emergency Teams
Recently, there is increased emphasis on the use of a dedicated in-hospital rapid response system (RRS) for early intervention in at-risk patients. There are two components of this system: (a) case recognition and team activation, and (b) the emergent medical response. Medical emergency teams (METs) are the response component of an RRS that has the capability of prescribing therapy, providing advance airway management, securing central venous access, and beginning ICU-level care at the bedside (284). These teams are often composed of experienced nurses and doctors with skills in critical care who are available 24 hours a day to seek out, assess, and manage patients who clinically pose a threat to develop cardiac arrest. Several small studies documented reduction in cardiac arrest rates with the use of METs (285,286), but a recent large clustered randomized study was not able to show any difference in cardiac arrest, unexpected death, and unplanned ICU admissions with the use of METs (287). Further studies are needed to evaluate the effectiveness and feasibility of METs.
Research Considerations
Research in patients with CA is extremely challenging. Most of the interventions need to be applied very quickly to be beneficial, which makes it hard for researchers to obtain institutional review board approval.
Ethical Considerations and Informed Consent
Obtaining consent from family is not always possible or practical at the time of cardiac arrest. Some researchers argue that presuming consent in these patients serves a benefit to the living and others argue that since the patient is clinically dead, consent is unnecessary since a dead patient is without autonomy. This argument does not account for the potential emotional harm to the family, who may oppose use of a deceased loved one for research, and also does not account for their cultural and religious beliefs.
Recently the importance of CPR research was recognized and the FDA adopted regulations that allow exception for consent in certain circumstances. Obtaining an exception requires the researcher to consult with experts in the field and representative lay persons, along with open and full public disclosure of the study, including the methodologic details of, need for, and benefit of the research.
References
1. Chugh SS, Jui J, Gunson K, et al. Current burden of sudden cardiac death: multiple source surveillance versus retrospective death certificate-based review in a large U.S. community. J Am Coll Cardiol. 2004;44(6):1268–1275.
2. Vaillancourt C, Stiell IG. Cardiac arrest care and emergency medical services in Canada. Can J Cardiol. 2004;20(11):1081–1090.
3. Valenzuela TD, Roe DJ, Cretin S, et al. Estimating effectiveness of cardiac arrest interventions: a logistic regression survival model. Circulation. 1997;96(10):3308–3313.
4. Nadkarni VM, Larkin GL, Peberdy MA, et al. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA. 2006;295(1):50–57.
5. Holmberg M, Holmberg S, Herlitz J. Effect of bystander cardiopulmonary resuscitation in out-of-hospital cardiac arrest patients in Sweden. Resuscitation. 2000;47(1):59–70.
6. Larsen MP, Eisenberg MS, Cummins RO, et al. Predicting survival from out-of-hospital cardiac arrest: a graphic model. Ann Emerg Med. 1993;22(11):1652–1658.
7. Callans DJ. Out-of-hospital cardiac arrest—the solution is shocking. N Engl J Med. 2004;351(7):632–634.
8. Wik L, Hansen TB, Fylling F, et al. Delaying defibrillation to give basic cardiopulmonary resuscitation to patients with out-of-hospital ventricular fibrillation: a randomized trial. JAMA. 2003;289(11):1389–1395.
9. Kellum MJ, Kennedy KW, Ewy GA. Cardiocerebral resuscitation improves survival of patients with out-of-hospital cardiac arrest. Am J Med. 2006;119(4):335–340.
10. 2005 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) of pediatric and neonatal patients: pediatric basic life support. Pediatrics. 2006;117(5):e989–1004.
11. Gasco Garcia MC, Rabanal Llevot JM. [New directives for basic and advanced cardiopulmonary resuscitation from the International Liaison Committee on Resuscitation (ILCOR). Directives of the European Resuscitation Council (ERC) for 2005.] Rev Esp Anestesiol Reanim. 2006;53(5):273–274.
12. The International Liaison Committee on Resuscitation (ILCOR) consensus on science with treatment recommendations for pediatric and neonatal patients: neonatal resuscitation. Pediatrics. 2006;117(5):e978–988.
13. Jacobs I, Nadkarni V, Bahr J, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update and simplification of the Utstein templates for resuscitation registries. A statement for healthcare professionals from a task force of the international liaison committee on resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa). Resuscitation. 2004;63(3):233–249.
14. Cummins RO. The Utstein style for uniform reporting of data from out-of-hospital cardiac arrest. Ann Emerg Med. 1993;22(1):37–40.
15. Cummins RO, Chamberlain D, Hazinski MF, et al. Recommended guidelines for reviewing, reporting, and conducting research on in-hospital resuscitation: the in-hospital ‘Utstein style’. A statement for healthcare professionals from the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, the Australian Resuscitation Council, and the Resuscitation Councils of Southern Africa. Resuscitation. 1997;34(2):151–183.
16. Zaritsky A, Nadkarni V, Hazinski MF, et al. Recommended guidelines for uniform reporting of pediatric advanced life support: the pediatric Utstein Style. A statement for healthcare professionals from a task force of the American Academy of Pediatrics, the American Heart Association, and the European Resuscitation Council. Writing Group. Circulation. 1995;92(7):2006–2020.
17. Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58(3):297–308.
18. Myerburg RJ, Fenster J, Velez M, et al. Impact of community-wide police car deployment of automated external defibrillators on survival from out-of-hospital cardiac arrest. Circulation. 2002;106(9):1058–1064.
19. Eisenburger P, Sterz F, Haugk M, et al. Cardiac arrest in public locations—an independent predictor for better outcome? Resuscitation. 2006;70(3):395–403.
20. Donoghue AJ, Nadkarni V, Berg RA, et al. Out-of-hospital pediatric cardiac arrest: an epidemiologic review and assessment of current knowledge. Ann Emerg Med. 2005;46(6):512–522.
21. Herlitz J, Bahr J, Fischer M, et al. Resuscitation in Europe: a tale of five European regions. Resuscitation. 1999;41(2):121–131.
22. Berger R, Kelley M. Survival after in-hospital cardiopulmonary arrest of noncritically ill patients. A prospective study. Chest. 1994;106(3):872–879.
23. Brindley PG, Markland DM, Mayers I, et al. Predictors of survival following in-hospital adult cardiopulmonary resuscitation. CMAJ. 2002;167(4):343–348.
24. Cohn AC, Wilson WM, Yan B, et al. Analysis of clinical outcomes following in-hospital adult cardiac arrest. Intern Med J. 2004;34(7):398–402.
25. Sandroni C, Ferro G, Santangelo S, et al. In-hospital cardiac arrest: survival depends mainly on the effectiveness of the emergency response. Resuscitation. 2004;62(3):291–297.
26. Samson RA, Nadkarni VM, Meaney PA, et al. Outcomes of in-hospital ventricular fibrillation in children. N Engl J Med. 2006;354(22):2328–2339.
27. Levy DE, Caronna JJ, Singer BH, et al. Predicting outcome from hypoxic-ischemic coma. JAMA. 1985;253(10):1420–1426.
28. Longstreth WT Jr, Diehr P, Inui TS. Prediction of awakening after out-of-hospital cardiac arrest. N Engl J Med. 1983;308(23):1378–1382.
29. Longstreth WT Jr, Inui TS, Cobb LA, et al. Neurologic recovery after out-of-hospital cardiac arrest. Ann Intern Med. 1983;98(5 Pt 1):588–592.
30. Gray WA, Capone RJ, Most AS. Unsuccessful emergency medical resuscitation—are continued efforts in the emergency department justified? N Engl J Med. 1991;325(20):1393–1398.
31. Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. 1975;1(7905):480–484.
32. A randomized clinical study of a calcium-entry blocker (lidoflazine) in the treatment of comatose survivors of cardiac arrest. Brain Resuscitation Clinical Trial II Study Group. N Engl J Med. 1991;324(18):1225–1231.
33. Safar PB, Bircher NG. Cardiopulmonary Cerebral Resuscitation: Basic and Advanced Cardiac and Trauma Life Support: An Introduction to Resuscitation Medicine. 3rd ed. London: W.B. Saunders; 1988.
34. Fiser DH. Assessing the outcome of pediatric intensive care. J Pediatr. 1992;121(1):68–74.
35. Fiser DH, Long N, Roberson PK, et al. Relationship of pediatric overall performance category and pediatric cerebral performance category scores at pediatric intensive care unit discharge with outcome measures collected at hospital discharge and 1- and 6-month follow-up assessments. Crit Care Med. 2000;28(7):2616–2620.
36. Fiser DH, Tilford JM, Roberson PK. Relationship of illness severity and length of stay to functional outcomes in the pediatric intensive care unit: a multi-institutional study. Crit Care Med. 2000;28(4):1173–1179.
37. Bottiger BW, Grabner C, Bauer H, et al. Long term outcome after out-of-hospital cardiac arrest with physician staffed emergency medical services: the Utstein style applied to a midsized urban/suburban area. Heart. 1999;82(6):674–679.
38. Westal RE, Reissman S, Doering G. Out-of-hospital cardiac arrests: an 8-year New York City experience. Am J Emerg Med. 1996;14(4):364–368.
39. Waalewijn RA, Nijpels MA, Tijssen JG, et al. Prevention of deterioration of ventricular fibrillation by basic life support during out-of-hospital cardiac arrest. Resuscitation. 2002;54(1):31–36.
40. Aufderheide TP, Lurie KG. Death by hyperventilation: a common and life-threatening problem during cardiopulmonary resuscitation. Crit Care Med. 2004;32(9 Suppl):S345–351.
41. Safar P, Escarraga LA, Chang F. Upper airway obstruction in the unconscious patient. J Appl Physiol. 1959;14:760–764.
42. Eberle B, Dick WF, Schneider T, et al. Checking the carotid pulse check: diagnostic accuracy of first responders in patients with and without a pulse. Resuscitation. 1996;33(2):107–116.
43. Ruppert M, Reith MW, Widmann JH, et al. Checking for breathing: evaluation of the diagnostic capability of emergency medical services personnel, physicians, medical students, and medical laypersons. Ann Emerg Med. 1999;34(6):720–729.
44. Lawrence PJ, Sivaneswaran N. Ventilation during cardiopulmonary resuscitation: which method? Med J Aust. 1985;143(10):443–446.
45. 2005 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Part 2: Adult basic life support. Resuscitation. 2005;67(2-3):187–201.
46. Johannigman JA, Branson RD, Davis K Jr, et al. Techniques of emergency ventilation: a model to evaluate tidal volume, airway pressure, and gastric insufflation. J Trauma. 1991;31(1):93–98.
47. McSwain GR, Garrison WB, Artz CP. Evaluation of resuscitation from cardiopulmonary arrest by paramedics. Ann Emerg Med. 1980;9(7):341–345.
48. Hess D, Baran C. Ventilatory volumes using mouth-to-mouth, mouth-to-mask, and bag-valve-mask techniques. Am J Emerg Med. 1985;3(4):292–296.
49. Jesudian MC, Harrison RR, Keenan RL, et al. Bag-valve-mask ventilation; two rescuers are better than one: preliminary report. Crit Care Med. 1985;13(2):122–123.
50. Campbell TP, Stewart RD, Kaplan RM, et al. Oxygen enrichment of bag-valve-mask units during positive-pressure ventilation: a comparison of various techniques. Ann Emerg Med. 1988;17(3):232–235.
51. Nam SH, Kim KJ, Nam YT, et al. The changes in delivered oxygen fractions using laerdal resuscitator bag with different types of reservoir. Yonsei Med J. 2001;42(2):242–246.
52. Hirschman AM, Kravath RE. Venting vs ventilating. A danger of manual resuscitation bags. Chest. 1982;82(3):369–370.
53. Lurie K, Zielinski T, McKnite S, et al. Improving the efficiency of cardiopulmonary resuscitation with an inspiratory impedance threshold valve. Crit Care Med. 2000;28(11 Suppl):N207–209.
54. Lurie KG, Mulligan KA, McKnite S, et al. Optimizing standard cardiopulmonary resuscitation with an inspiratory impedance threshold valve. Chest. 1998;113(4):1084–1090.
55. Sigurdsson G, Yannopoulos D, McKnite SH, et al. Effects of an inspiratory impedance threshold device on blood pressure and short term survival in spontaneously breathing hypovolemic pigs. Resuscitation. 2006;68(3):399–404.
56. Bahr J, Klingler H, Panzer W, et al. Skills of lay people in checking the carotid pulse. Resuscitation. 1997;35(1):23–26.
57. Moule P. Checking the carotid pulse: diagnostic accuracy in students of the healthcare professions. Resuscitation. 2000;44(3):195–201.
58. Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 3: adult basic life support. The American Heart Association in collaboration with the International Liaison Committee on Resuscitation. Circulation. 2000;102(8 Suppl):I22–59.
59. Keen WW. Case of total laryngectomy (unsuccessful) and a case of abdomen hysterectomy (successful) in both which massage of the heart for chloroform collapse was employed, with notes of 25 other cases of cardiac massage. Ther Gaz. 1904;28:217–220.
60. Lee WE, Downs TM. Resuscitation by direct massage of the heart in the cardiac arrest. Ann Surg. 1924;80:555–561.
61. Bircher N, Safar P. Manual open-chest cardiopulmonary resuscitation. Ann Emerg Med. 1984;13(9 Pt 2):770–773.
62. Ewer MS, Ali MK, Frazier OH. Open chest resuscitation for cardiopulmonary arrest related to mechanical impairment of circulation: a report of two cases. Crit Care Med. 1982;10(3):198–199.
63. Alifimoff JK. Open versus closed chest cardiac massage in non-traumatic cardiac arrest. Resuscitation. 1987;15(1):13–21.
64. Robertson C. Open-chest cardiac massage for non-traumatic cardiac arrest. Arch Emerg Med. 1987;4(4):207–210.
65. Boczar ME, Howard MA, Rivers EP, et al. A technique revisited: hemodynamic comparison of closed- and open-chest cardiac massage during human cardiopulmonary resuscitation. Crit Care Med. 1995;23(3):498–503.
66. Pottle A, Bullock I, Thomas J, et al. Survival to discharge following open chest cardiac compression (OCCC). A 4-year retrospective audit in a cardiothoracic specialist centre–Royal Brompton and Harefield NHS Trust, United Kingdom. Resuscitation. 2002;52(3):269–272.
67. Raman J, Saldanha RF, Branch JM, et al. Open cardiac compression in the postoperative cardiac intensive care unit. Anaesth Intensive Care. 1989;17(2):129–135.
68. Geehr EC, Lewis FR, Auerbach PS. Failure of open-heart massage to improve survival after prehospital nontraumatic cardiac arrest. N Engl J Med. 1986;314(18):1189–1190.
69. Kouwenhoven WB, Jude JR, Knickerbocker GG. Closed-chest cardiac massage. JAMA. 1960;173:1064–1067.
70. Jude JR, Kouwenhoven WB, Knickerbocker GG. Cardiac arrest. Report of application of external cardiac massage on 118 patients. JAMA. 1961;178:1063–1070.
71. Criley JM, Blaufuss AH, Kissel GL. Cough-induced cardiac compression. Self-administered from of cardiopulmonary resuscitation. JAMA. 1976;236(11):1246–1250.
72. Criley JM, Blaufuss AH, Kissel GL. Self-administered cardiopulmonary resuscitation by cough-induced cardiac compression. Trans Am Clin Climatol Assoc. 1976;87:138–146.
73. Chandra N, Rudikoff M, Weisfeldt ML. Simultaneous chest compression and ventilation at high airway pressure during cardiopulmonary resuscitation. Lancet. 1980;1(8161):175–178.
74. Rudikoff MT, Maughan WL, Effron M, et al. Mechanisms of blood flow during cardiopulmonary resuscitation. Circulation. 1980;61(2):345–352.
75. Rich S, Wix HL, Shapiro EP. Clinical assessment of heart chamber size and valve motion during cardiopulmonary resuscitation by two-dimensional echocardiography. Am Heart J. 1981;102(3 Pt 1):368–373.
76. Werner JA, Greene HL, Janko CL, et al. Two-dimensional echocardiography during CPR in man: implications regarding the mechanism of blood flow. Crit Care Med. 1981;9(5):375–376.
77. Deshmukh HG, Weil MH, Gudipati CV, et al. Mechanism of blood flow generated by precordial compression during CPR. I. Studies on closed chest precordial compression. Chest. 1989;95(5):1092–1099.
78. Orlowski JP. Optimum position for external cardiac compression in infants and young children. Ann Emerg Med. 1986;15(6):667–673.
79. Paradis NA, Martin GB, Goetting MG, et al. Simultaneous aortic, jugular bulb, and right atrial pressures during cardiopulmonary resuscitation in humans. Insights into mechanisms. Circulation. 1989;80(2):361–368.
80. Tweed M, Tweed C, Perkins GD. The effect of differing support surfaces on the efficacy of chest compressions using a resuscitation manikin model. Resuscitation. 2001;51(2):179–183.
81. Handley AJ, Handley JA. Performing chest compressions in a confined space. Resuscitation. 2004;61(1):55–61.
82. Perkins GD, Stephenson BT, Smith CM, et al. A comparison between over-the-head and standard cardiopulmonary resuscitation. Resuscitation. 2004;61(2):155–161.
83. Handley AJ. Teaching hand placement for chest compression—a simpler technique. Resuscitation. 2002;53(1):29–36.
84. Kundra P, Dey S, Ravishankar M. Role of dominant hand position during external cardiac compression. Br J Anaesth. 2000;84(4):491–493.
85. Aufderheide TP, Pirrallo RG, Yannopoulos D, et al. Incomplete chest wall decompression: a clinical evaluation of CPR performance by EMS personnel and assessment of alternative manual chest compression-decompression techniques. Resuscitation. 2005;64(3):353–362.
86. Yannopoulos D, McKnite S, Aufderheide TP, et al. Effects of incomplete chest wall decompression during cardiopulmonary resuscitation on coronary and cerebral perfusion pressures in a porcine model of cardiac arrest. Resuscitation. 2005;64(3):363–372.
87. Stevenson AG, McGowan J, Evans AL, et al. CPR for children: one hand or two? Resuscitation. 2005;64(2):205–208.
88. Clements F, McGowan J. Finger position for chest compressions in cardiac arrest in infants. Resuscitation. 2000;44(1):43–46.
89. Finholt DA, Kettrick RG, Wagner HR, et al. The heart is under the lower third of the sternum. Implications for external cardiac massage. Am J Dis Child. 1986;140(7):646–649.
90. Shah NM, Gaur HK. Position of heart in relation to sternum and nipple line at various ages. Indian Pediatr. 1992;29(1):49–53.
91. Houri PK, Frank LR, Menegazzi JJ, et al. A randomized, controlled trial of two-thumb vs two-finger chest compression in a swine infant model of cardiac arrest [see comment]. Prehosp Emerg Care. 1997;1(2):65–67.
92. Dorfsman ML, Menegazzi JJ, Wadas RJ, et al. Two-thumb vs. two-finger chest compression in an infant model of prolonged cardiopulmonary resuscitation. Acad Emerg Med. 2000;7(10):1077–1082.
93. Whitelaw CC, Slywka B, Goldsmith LJ. Comparison of a two-finger versus two-thumb method for chest compressions by healthcare providers in an infant mechanical model. Resuscitation. 2000;43(3):213–216.
94. Wik L, Kramer-Johansen J, Myklebust H, et al. Quality of cardiopulmonary resuscitation during out-of-hospital cardiac arrest. JAMA. 2005;293(3):299–304.
95. Abella BS, Alvarado JP, Myklebust H, et al. Quality of cardiopulmonary resuscitation during in-hospital cardiac arrest. JAMA. 2005;293(3):305–310.
96. Yu T, Weil MH, Tang W, et al. Adverse outcomes of interrupted precordial compression during automated defibrillation. Circulation. 2002;106(3):368–372.
97. Swenson RD, Weaver WD, Niskanen RA, et al. Hemodynamics in humans during conventional and experimental methods of cardiopulmonary resuscitation. Circulation. 1988;78(3):630–639.
98. Kern KB, Sanders AB, Raife J, et al. A study of chest compression rates during cardiopulmonary resuscitation in humans. The importance of rate-directed chest compressions. Arch Intern Med. 1992;152(1):145–149.
99. Halperin HR, Tsitlik JE, Guerci AD, et al. Determinants of blood flow to vital organs during cardiopulmonary resuscitation in dogs. Circulation. 1986;73(3):539–550.
100. Feneley MP, Maier GW, Kern KB, et al. Influence of compression rate on initial success of resuscitation and 24 hour survival after prolonged manual cardiopulmonary resuscitation in dogs. Circulation. 1988;77(1):240–250.
101. Handley AJ, Handley JA. The relationship between rate of chest compression and compression:relaxation ratio. Resuscitation. 1995;30(3):237–241.
102. Rea TD, Helbock M, Perry S, et al. Increasing use of cardiopulmonary resuscitation during out-of-hospital ventricular fibrillation arrest: survival implications of guideline changes. Circulation. 2006;114(25):2760–2765.
103. Aufderheide TP, Sigurdsson G, Pirrallo RG, et al. Hyperventilation-induced hypotension during cardiopulmonary resuscitation. Circulation. 2004;109(16):1960–1965.
104. Greingor JL. Quality of cardiac massage with ratio compression-ventilation 5/1 and 15/2. Resuscitation. 2002;55(3):263–267.
105. Odegaard S, Saether E, Steen AS, et al. Quality of lay person CPR performance with compression:ventilation ratios 15:2, 30:2 or continuous chest compressions without ventilations on maikins. Resuscitation. 2006;doi10.1016/j.resuscitation.2006.05.012.
106. Beyar R, Kishon Y, Kimmel E, et al. Intrathoracic and abdominal pressure variations as an efficient method for cardiopulmonary resuscitation: studies in dogs compared with computer model results. Cardiovasc Res. 1985;19(6):335–342.
107. Voorhees WD, Niebauer MJ, Babbs CF. Improved oxygen delivery during cardiopulmonary resuscitation with interposed abdominal compressions. Ann Emerg Med. 1983;12(3):128–135.
108. Sack JB, Kesselbrenner MB, Jarrad A. Interposed abdominal compression-cardiopulmonary resuscitation and resuscitation outcome during asystole and electromechanical dissociation. Circulation. 1992;86(6):1692–1700.
109. Sack JB, Kesselbrenner MB, Bregman D. Survival from in-hospital cardiac arrest with interposed abdominal counterpulsation during cardiopulmonary resuscitation. JAMA. 1992;267(3):379–385.
110. Lurie KG, Shultz JJ, Callaham ML, et al. Evaluation of active compression-decompression CPR in victims of out-of-hospital cardiac arrest. JAMA 1994;271(18):1405–1411.
111. Plaisance P, Lurie KG, Vicaut E, et al. A comparison of standard cardiopulmonary resuscitation and active compression-decompression resuscitation for out-of-hospital cardiac arrest. French Active Compression-Decompression Cardiopulmonary Resuscitation Study Group. N Engl J Med. 1999;341(8):569–575.
112. Tucker KJ, Galli F, Savitt MA, et al. Active compression-decompression resuscitation: effect on resuscitation success after in-hospital cardiac arrest. J Am Coll Cardiol. 1994;24(1):201–209.
113. Schwab TM, Callaham ML, Madsen CD, et al. A randomized clinical trial of active compression-decompression CPR vs standard CPR in out-of-hospital cardiac arrest in two cities. JAMA. 1995;273(16):1261–1268.
114. Stiell IG, Hebert PC, Wells GA, et al. The Ontario trial of active compression-decompression cardiopulmonary resuscitation for in-hospital and prehospital cardiac arrest. JAMA. 1996;275(18):1417–1423.
115. Mauer D, Schneider T, Dick W, et al. Active compression-decompression resuscitation: a prospective, randomized study in a two-tiered EMS system with physicians in the field. Resuscitation. 1996;33(2):125–134.
116. Luiz T, Ellinger K, Denz C. Active compression-decompression cardiopulmonary resuscitation does not improve survival in patients with prehospital cardiac arrest in a physician-manned emergency medical system. J Cardiothorac Vasc Anesth. 1996;10(2):178–186.
117. Arntz HR, Agrawal R, Richter H, et al. Phased chest and abdominal compression-decompression versus conventional cardiopulmonary resuscitation in out-of-hospital cardiac arrest. Circulation. 2001;104(7):768–772.
118. Dickinson ET, Verdile VP, Schneider RM, et al. Effectiveness of mechanical versus manual chest compressions in out-of-hospital cardiac arrest resuscitation: a pilot study. Am J Emerg Med. 1998;16(3):289–292.
119. McDonald JL. Systolic and mean arterial pressures during manual and mechanical CPR in humans. Ann Emerg Med. 1982;11(6):292–295.
120. Ward KR, Menegazzi JJ, Zelenak RR, et al. A comparison of chest compressions between mechanical and manual CPR by monitoring end-tidal PCO2 during human cardiac arrest. Ann Emerg Med. 1993;22(4):669–674.
121. Casner M, Andersen D, Isaacs SM. The impact of a new CPR assist device on rate of return of spontaneous circulation in out-of-hospital cardiac arrest. Prehosp Emerg Care. 2005;9(1):61–67.
122. Ong ME, Ornato JP, Edwards DP, et al. Use of an automated, load-distributing band chest compression device for out-of-hospital cardiac arrest resuscitation. JAMA. 2006;295(22):2629–2637.
123. Hallstrom A, Rea TD, Sayre MR, et al. Manual chest compression vs use of an automated chest compression device during resuscitation following out-of-hospital cardiac arrest: a randomized trial. JAMA. 2006;295(22):2620–2628.
124. Pepe PE, Copass MK, Joyce TH. Prehospital endotracheal intubation: rationale for training emergency medical personnel. Ann Emerg Med. 1985;14(11):1085–1092.
125. Gausche M, Lewis RJ, Stratton SJ, et al. Effect of out-of-hospital pediatric endotracheal intubation on survival and neurological outcome: a controlled clinical trial. JAMA. 2000;283(6):783–790.
126. Jones JH, Murphy MP, Dickson RL, et al. Emergency physician-verified out-of-hospital intubation: miss rates by paramedics. Acad Emerg Med. 2004;11(6):707–709.
127. Sayre MR, Sakles JC, Mistler AF, et al. Field trial of endotracheal intubation by basic EMTs. Ann Emerg Med. 1998;31(2):228–233.
128. Katz SH, Falk JL. Misplaced endotracheal tubes by paramedics in an urban emergency medical services system. Ann Emerg Med. 2001;37(1):32–37.
129. Bhende MS, Thompson AE, Cook DR, et al. Validity of a disposable end-tidal CO2 detector in verifying endotracheal tube placement in infants and children. Ann Emerg Med. 1992;21(2):142–145.
130. Ornato JP, Shipley JB, Racht EM, et al. Multicenter study of a portable, hand-size, colorimetric end-tidal carbon dioxide detection device. Ann Emerg Med. 1992;21(5):518–523.
131. Vukmir RB, Heller MB, Stein KL. Confirmation of endotracheal tube placement: a miniaturized infrared qualitative CO2 detector. Ann Emerg Med. 1991;20(7):726–729.
132. 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2005;112(24 Suppl):IV1–203.
133. Bozeman WP, Hexter D, Liang HK, et al. Esophageal detector device versus detection of end-tidal carbon dioxide level in emergency intubation. Ann Emerg Med. 1996;27(5):595–599.
134. Sharieff GQ, Rodarte A, Wilton N, et al. The self-inflating bulb as an airway adjunct: is it reliable in children weighing less than 20 kilograms? Acad Emerg Med. 2003;10(4):303–308.
135. Williams KN, Nunn JF. The oesophageal detector device. A prospective trial on 100 patients. Anaesthesia. 1989;44(5):412–414.
136. Haynes SR, Morton NS. Use of the oesophageal detector device in children under one year of age. Anaesthesia. 1990;45(12):1067–1069.
137. Capucci A, Aschieri D, Piepoli MF, et al. Tripling survival from sudden cardiac arrest via early defibrillation without traditional education in cardiopulmonary resuscitation. Circulation. 2002;106(9):1065–1070.
138. Holmberg M, Holmberg S, Herlitz J. Incidence, duration and survival of ventricular fibrillation in out-of-hospital cardiac arrest patients in Sweden. Resuscitation. 2000;44(1):7–17.
139. White RD, Hankins DG, Bugliosi TF. Seven years' experience with early defibrillation by police and paramedics in an emergency medical services system. Resuscitation. 1998;39(3):145–151.
140. Culley LL, Rea TD, Murray JA, et al. Public access defibrillation in out-of-hospital cardiac arrest: a community-based study. Circulation. 2004;109(15):1859–1863.
141. Skogvoll E, Isern E, Sangolt GK, et al. In-hospital cardiopulmonary resuscitation. 5 years' incidence and survival according to the Utstein template. Acta Anaesthesiol Scand. 1999;43(2):177–184.
142. Parish DC, Dane FC, Montgomery M, et al. Resuscitation in the hospital: relationship of year and rhythm to outcome. Resuscitation. 2000;47(3):219–229.
143. Cooper S, Cade J. Predicting survival, in-hospital cardiac arrests: resuscitation survival variables and training effectiveness. Resuscitation. 1997;35(1):17–22.
144. Andreasson AC, Herlitz J, Bang A, et al. Characteristics and outcome among patients with a suspected in-hospital cardiac arrest. Resuscitation. 1998;39(1–2):23–31.
145. White RD. External defibrillation: the need for uniformity in analyzing and reporting results. Ann Emerg Med. 1998;32(2):234–236.
146. Gliner BE, White RD. Electrocardiographic evaluation of defibrillation shocks delivered to out-of-hospital sudden cardiac arrest patients. Resuscitation. 1999;41(2):133–144.
147. Zhang Y, Rhee B, Davies LR, et al. Quadriphasic waveforms are superior to triphasic waveforms for transthoracic defibrillation in a cardiac arrest swine model with high impedance. Resuscitation. 2006;68(2):251–258.
148. Zhang Y, Ramabadran RS, Boddicker KA, et al. Triphasic waveforms are superior to biphasic waveforms for transthoracic defibrillation: experimental studies. J Am Coll Cardiol. 2003;42(3):568–575.
149. van Alem AP, Chapman FW, Lank P, et al. A prospective, randomised and blinded comparison of first shock success of monophasic and biphasic waveforms in out-of-hospital cardiac arrest. Resuscitation. 2003;58(1):17–24.
150. Schneider T, Martens PR, Paschen H, et al. Multicenter, randomized, controlled trial of 150-J biphasic shocks compared with 200- to 360-J monophasic shocks in the resuscitation of out-of-hospital cardiac arrest victims. Optimized Response to Cardiac Arrest (ORCA) Investigators. Circulation. 2000;102(15):1780–1787.
151. Morrison LJ, Dorian P, Long J, et al. Out-of-hospital cardiac arrest rectilinear biphasic to monophasic damped sine defibrillation waveforms with advanced life support intervention trial (ORBIT). Resuscitation. 2005;66(2):149–157.
152. Walsh SJ, McClelland AJ, Owens CG, et al. Efficacy of distinct energy delivery protocols comparing two biphasic defibrillators for cardiac arrest. Am J Cardiol. 2004;94(3):378–380.
153. Higgins SL, O'Grady SG, Banville I, et al. Efficacy of lower-energy biphasic shocks for transthoracic defibrillation: a follow-up clinical study. Prehosp Emerg Care. 2004;8(3):262–267.
154. Bourland JD, Tacker WA Jr, Geddes LA. Strength-duration curves for trapezoidal waveforms of various tilts for transchest defibrillation in animals. Med Instrum. 1978;12(1):38–41.
155. Bourland JD, Tacker WA Jr, Geddes LA, et al. Comparative efficacy of damped sine wave and square wave current for transchest ventricular defibrillation in animals. Med Instrum. 1978;12(1):42–45.
156. Kerber RE, Grayzel J, Hoyt R, et al. Transthoracic resistance in human defibrillation. Influence of body weight, chest size, serial shocks, paddle size and paddle contact pressure. Circulation. 1981;63(3):676–682.
157. Kerber RE, Kouba C, Martins J, et al. Advance prediction of transthoracic impedance in human defibrillation and cardioversion: importance of impedance in determining the success of low-energy shocks. Circulation. 1984;70(2):303–308.
158. Lerman BB, DiMarco JP, Haines DE. Current-based versus energy-based ventricular defibrillation: a prospective study. J Am Coll Cardiol. 1988;12(5):1259–1264.
159. Gurnett CA, Atkins DL. Successful use of a biphasic waveform automated external defibrillator in a high-risk child. Am J Cardiol. 2000;86(9):1051–1053.
160. Atkins DL, Jorgenson DB. Attenuated pediatric electrode pads for automated external defibrillator use in children. Resuscitation. 2005;66(1):31–37.
161. Berg RA, Chapman FW, Berg MD, et al. Attenuated adult biphasic shocks compared with weight-based monophasic shocks in a swine model of prolonged pediatric ventricular fibrillation. Resuscitation. 2004;61(2):189–197.
162. Cummins RO, Eisenberg M, Bergner L, et al. Sensitivity, accuracy, and safety of an automatic external defibrillator. Lancet. 1984;2(8398):318–320.
163. White RD, Vukov LF, Bugliosi TF. Early defibrillation by police: initial experience with measurement of critical time intervals and patient outcome. Ann Emerg Med. 1994;23(5):1009–1013.
164. Davis EA, Mosesso VN Jr. Performance of police first responders in utilizing automated external defibrillation on victims of sudden cardiac arrest. Prehosp Emerg Care. 1998;2(2):101–107.
165. Hallstrom AP, Ornato JP, Weisfeldt M, et al. Public-access defibrillation and survival after out-of-hospital cardiac arrest. N Engl J Med. 2004;351(7):637–646.
166. Sirna SJ, Ferguson DW, Charbonnier F, et al. Factors affecting transthoracic impedance during electrical cardioversion. Am J Cardiol. 1988;62(16):1048–1052.
167. Kerber RE, Martins JB, Kienzle MG, et al. Energy, current, and success in defibrillation and cardioversion: clinical studies using an automated impedance-based method of energy adjustment. Circulation. 1988;77(5):1038–1046.
168. Kerber RE, Kienzle MG, Olshansky B, et al. Ventricular tachycardia rate and morphology determine energy and current requirements for transthoracic cardioversion. Circulation. 1992;85(1):158–163.
169. Barthell E, Troiano P, Olson D, et al. Prehospital external cardiac pacing: a prospective, controlled clinical trial. Ann Emerg Med. 1988;17(11):1221–1226.
170. Cummins RO, Graves JR, Larsen MP, et al. Out-of-hospital transcutaneous pacing by emergency medical technicians in patients with asystolic cardiac arrest. N Engl J Med. 1993;328(19):1377–1382.
171. van Walraven C, Stiell IG, Wells GA, et al. Do advanced cardiac life support drugs increase resuscitation rates from in-hospital cardiac arrest? The OTAC Study Group. Ann Emerg Med. 1998;32(5):544–553.
172. Guy J, Haley K, Zuspan SJ. Use of intraosseous infusion in the pediatric trauma patient. J Pediatr Surg. 1993;28(2):158–161.
173. Banerjee S, Singhi SC, Singh S, et al. The intraosseous route is a suitable alternative to intravenous route for fluid resuscitation in severely dehydrated children. Indian Pediatr. 1994;31(12):1511–1520.
P.719
174. Glaeser PW, Hellmich TR, Szewczuga D, et al. Five-year experience in prehospital intraosseous infusions in children and adults. Ann Emerg Med. 1993;22(7):1119–1124.
175. Efrati O, Ben-Abraham R, Barak A, et al. Endobronchial adrenaline: should it be reconsidered? Dose response and haemodynamic effect in dogs. Resuscitation. 2003;59(1):117–122.
176. Manisterski Y, Vaknin Z, Ben-Abraham R, et al. Endotracheal epinephrine: a call for larger doses. Anesth Analg. 2002;95(4):1037–1041, table of contents.
177. Hilwig RW, Kern KB, Berg RA, et al. Catecholamines in cardiac arrest: role of alpha agonists, beta-adrenergic blockers and high-dose epinephrine. Resuscitation. 2000;47(2):203–208.
178. Chase PB, Kern KB, Sanders AB, et al. Effects of graded doses of epinephrine on both noninvasive and invasive measures of myocardial perfusion and blood flow during cardiopulmonary resuscitation. Crit Care Med. 1993;21(3):413–419.
179. Berg RA, Otto CW, Kern KB, et al. A randomized, blinded trial of high-dose epinephrine versus standard-dose epinephrine in a swine model of pediatric asphyxial cardiac arrest. Crit Care Med. 1996;24(10):1695–1700.
180. Berg RA, Otto CW, Kern KB, et al. High-dose epinephrine results in greater early mortality after resuscitation from prolonged cardiac arrest in pigs: a prospective, randomized study. Crit Care Med. 1994;22(2):282–290.
181. Gueugniaud PY, Mols P, Goldstein P, et al. A comparison of repeated high doses and repeated standard doses of epinephrine for cardiac arrest outside the hospital. European Epinephrine Study Group. N Engl J Med. 1998;339(22):1595–1601.
182. Vandycke C, Martens P. High dose versus standard dose epinephrine in cardiac arrest - a meta-analysis. Resuscitation. 2000;45(3):161–166.
183. Perondi MB, Reis AG, Paiva EF, et al. A comparison of high-dose and standard-dose epinephrine in children with cardiac arrest. N Engl J Med. 2004;350(17):1722–1730.
184. Krismer AC, Lindner KH, Wenzel V, et al. The effects of endogenous and exogenous vasopressin during experimental cardiopulmonary resuscitation. Anesth Analg. 2001;92(6):1499–1504.
185. Stiell IG, Hebert PC, Wells GA, et al. Vasopressin versus epinephrine for inhospital cardiac arrest: a randomised controlled trial. Lancet. 2001;358(9276):105–109.
186. Wenzel V, Krismer AC, Arntz HR, et al. A comparison of vasopressin and epinephrine for out-of-hospital cardiopulmonary resuscitation. N Engl J Med. 2004;350(2):105–113.
187. Aung K, Htay T. Vasopressin for cardiac arrest: a systematic review and meta-analysis. Arch Intern Med. 2005;165(1):17–24.
188. Voelckel WG, Lurie KG, McKnite S, et al. Comparison of epinephrine and vasopressin in a pediatric porcine model of asphyxial cardiac arrest. Crit Care Med. 2000;28(12):3777–3783.
189. Kette F, Weil MH, Gazmuri RJ. Buffer solutions may compromise cardiac resuscitation by reducing coronary perfusion pressure. JAMA. 1991;266(15):2121–2126.
190. Graf H, Leach W, Arieff AI. Evidence for a detrimental effect of bicarbonate therapy in hypoxic lactic acidosis. Science. 1985;227(4688):754–756.
191. Benjamin E, Oropello JM, Abalos AM, et al. Effects of acid-base correction on hemodynamics, oxygen dynamics, and resuscitability in severe canine hemorrhagic shock. Crit Care Med. 1994;22(10):1616–1623.
192. Gunnar RM, Passamani ER, Bourdillon PD, et al. Guidelines for the early management of patients with acute myocardial infarction. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee to Develop Guidelines for the Early Management of Patients with Acute Myocardial Infarction). J Am Coll Cardiol. 1990;16(2):249–292.
193. Paradis NA, Martin GB, Rivers EP, et al. Coronary perfusion pressure and the return of spontaneous circulation in human cardiopulmonary resuscitation. JAMA. 1990;263(8):1106–1113.
194. Marill KA, Greenberg GM, Kay D, et al. Analysis of the treatment of spontaneous sustained stable ventricular tachycardia. Acad Emerg Med. 1997;4(12):1122–1128.
195. Somberg JC, Bailin SJ, Haffajee CI, et al. Intravenous lidocaine versus intravenous amiodarone (in a new aqueous formulation) for incessant ventricular tachycardia. Am J Cardiol. 2002;90(8):853–859.
196. Gorgels AP, van den Dool A, Hofs A, et al. Comparison of procainamide and lidocaine in terminating sustained monomorphic ventricular tachycardia. Am J Cardiol. 1996;78(1):43–46.
197. Schutzenberger W, Leisch F, Kerschner K, et al. Clinical efficacy of intravenous amiodarone in the short term treatment of recurrent sustained ventricular tachycardia and ventricular fibrillation. Br Heart J. 1989;62(5):367–371.
198. Cybulski J, Kulakowski P, Makowska E, et al. Intravenous amiodarone is safe and seems to be effective in termination of paroxysmal supraventricular tachyarrhythmias. Clin Cardiol. 1996;19(7):563–566.
199. Cotter G, Blatt A, Kaluski E, et al. Conversion of recent onset paroxysmal atrial fibrillation to normal sinus rhythm: the effect of no treatment and high-dose amiodarone. A randomized, placebo-controlled study. Eur Heart J. 1999;20(24):1833–1842.
200. Stueven HA, Thompson B, Aprahamian C, et al. The effectiveness of calcium chloride in refractory electromechanical dissociation. Ann Emerg Med. 1985;14(7):626–629.
201. Stueven HA, Thompson B, Aprahamian C, et al. Lack of effectiveness of calcium chloride in refractory asystole. Ann Emerg Med. 1985;14(7):630–632.
202. Fatovich DM, Prentice DA, Dobb GJ. Magnesium in cardiac arrest (the magic trial). Resuscitation. 1997;35(3):237–241.
203. Miller B, Craddock L, Hoffenberg S, et al. Pilot study of intravenous magnesium sulfate in refractory cardiac arrest: safety data and recommendations for future studies. Resuscitation. 1995;30(1):3–14.
204. Connick M, Berg RA. Femoral venous pulsations during open-chest cardiac massage. Ann Emerg Med. 1994;24(6):1176–1179.
205. Halperin HR, Tsitlik JE, Gelfand M, et al. A preliminary study of cardiopulmonary resuscitation by circumferential compression of the chest with use of a pneumatic vest. N Engl J Med. 1993;329(11):762–768.
206. Kern KB, Ewy GA, Voorhees WD, et al. Myocardial perfusion pressure: a predictor of 24-hour survival during prolonged cardiac arrest in dogs. Resuscitation. 1988;16(4):241–250.
207. Weil MH, Rackow EC, Trevino R, et al. Difference in acid-base state between venous and arterial blood during cardiopulmonary resuscitation. N Engl J Med. 1986;315(3):153–156.
208. Kette F, Weil MH, Gazmuri RJ, et al. Intramyocardial hypercarbic acidosis during cardiac arrest and resuscitation. Crit Care Med. 1993;21(6):901–906.
209. Tucker KJ, Idris AH, Wenzel V, et al. Changes in arterial and mixed venous blood gases during untreated ventricular fibrillation and cardiopulmonary resuscitation. Resuscitation. 1994;28(2):137–141.
210. Gudipati CV, Weil MH, Gazmuri RJ, et al. Increases in coronary vein CO2 during cardiac resuscitation. J Appl Physiol. 1990;68(4):1405–1408.
211. Bircher NG. Acidosis of cardiopulmonary resuscitation: carbon dioxide transport and anaerobiosis. Crit Care Med. 1992;20(9):1203–1205.
212. Gravenstein JS, Paulus DA, Hayes TJ, et al. Capnography in Clinical Practice. Boston: Butterworths; 1989.
213. Idris AH, Staples ED, O'Brien DJ, et al. End-tidal carbon dioxide during extremely low cardiac output. Ann Emerg Med. 1994;23(3):568–572.
214. Gazmuri RJ, Weil MH, Bisera J, et al. End-tidal carbon dioxide tension as a monitor of native blood flow during resuscitation by extracorporeal circulation. J Thorac Cardiovasc Surg. 1991;101(6):984–988.
215. Gudipati CV, Weil MH, Bisera J, et al. Expired carbon dioxide: a noninvasive monitor of cardiopulmonary resuscitation. Circulation. 1988;77(1):234–239.
216. Sanders AB, Atlas M, Ewy GA, et al. Expired PCO2 as an index of coronary perfusion pressure. Am J Emerg Med. 1985;3(2):147–149.
217. Falk JL, Rackow EC, Weil MH. End-tidal carbon dioxide concentration during cardiopulmonary resuscitation. N Engl J Med. 1988;318(10):607–611.
218. Sanders AB, Kern KB, Otto CW, et al. End-tidal carbon dioxide monitoring during cardiopulmonary resuscitation. A prognostic indicator for survival. JAMA. 1989;262(10):1347–1351.
219. Wiklund L, Soderberg D, Henneberg S, et al. Kinetics of carbon dioxide during cardiopulmonary resuscitation. Crit Care Med. 1986;14(12):1015–1022.
220. Callaham M, Barton C. Prediction of outcome of cardiopulmonary resuscitation from end-tidal carbon dioxide concentration. Crit Care Med. 1990;18(4):358–362.
221. Bhende MS, Thompson AE. Evaluation of an end-tidal CO2 detector during pediatric cardiopulmonary resuscitation. Pediatrics. 1995;95(3):395–399.
222. Ornato JP, Gonzalez ER, Garnett AR, et al. Effect of cardiopulmonary resuscitation compression rate on end-tidal carbon dioxide concentration and arterial pressure in man. Crit Care Med. 1988;16(3):241–245.
223. Ornato JP, Levine RL, Young DS, et al. The effect of applied chest compression force on systemic arterial pressure and end-tidal carbon dioxide concentration during CPR in human beings. Ann Emerg Med. 1989;18(7):732–737.
224. Martin GB, Gentile NT, Paradis NA, et al. Effect of epinephrine on end-tidal carbon dioxide monitoring during CPR. Ann Emerg Med. 1990;19(4):396–398.
225. Sanders AB, Ewy GA, Bragg S, et al. Expired PCO2 as a prognostic indicator of successful resuscitation from cardiac arrest. Ann Emerg Med. 1985;14(10):948–952.
226. Idris AH, Staples ED, O'Brien DJ, et al. Effect of ventilation on acid-base balance and oxygenation in low blood-flow states. Crit Care Med. 1994;22(11):1827–1834.
227. Laurent I, Monchi M, Chiche JD, et al. Reversible myocardial dysfunction in survivors of out-of-hospital cardiac arrest. J Am Coll Cardiol. 2002;40(12):2110–2116.
228. Negovsky VA. The second step in resuscitation—the treatment of the ‘post-resuscitation disease’. Resuscitation. 1972;1(1):1–7.
229. Safar P. Resuscitation from clinical death: pathophysiologic limits and therapeutic potentials. Crit Care Med. 1988;16(10):923–941.
230. Skrifvars MB, Pettila V, Rosenberg PH, et al. A multiple logistic regression analysis of in-hospital factors related to survival at six months in patients resuscitated from out-of-hospital ventricular fibrillation. Resuscitation. 2003;59(3):319–328.
231. Longstreth WT Jr, Inui TS. High blood glucose level on hospital admission and poor neurological recovery after cardiac arrest. Ann Neurol. 1984;15(1):59–63.
232. Calle PA, Buylaert WA, Vanhaute OA. Glycemia in the post-resuscitation period. The Cerebral Resuscitation Study Group. Resuscitation. 1989;17(Suppl):S181–188; discussion S199–206.
233. Longstreth WT Jr, Copass MK, Dennis LK, et al. Intravenous glucose after out-of-hospital cardiopulmonary arrest: a community-based randomized trial. Neurology. 1993;43(12):2534–2541.
234. van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345(19):1359–1367.
235. Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006;354(5):449–461.
236. Weaver WD, Cobb LA, Copass MK, et al. Ventricular defibrillation—a comparative trial using 175-J and 320-J shocks. N Engl J Med. 1982;307(18):1101–1106.
237. Kern KB, Hilwig RW, Rhee KH, et al. Myocardial dysfunction after resuscitation from cardiac arrest: an example of global myocardial stunning. J Am Coll Cardiol. 1996;28(1):232–240.
238. Adrie C, Adib-Conquy M, Laurent I, et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation. 2002;106(5):562–568.
239. Gisvold SE, Sterz F, Abramson NS, et al. Cerebral resuscitation from cardiac arrest: treatment potentials. Crit Care Med. 1996;24(2 Suppl):S69–80.
240. del Zoppo GJ, Mabuchi T. Cerebral microvessel responses to focal ischemia. J Cereb Blood Flow Metab. 2003;23(8):879–894.
241. Hickey RW, Kochanek PM, Ferimer H, et al. Induced hyperthermia exacerbates neurologic neuronal histologic damage after asphyxial cardiac arrest in rats. Crit Care Med. 2003;31(2):531–535.
242. Dietrich WD, Busto R, Halley M, et al. The importance of brain temperature in alterations of the blood-brain barrier following cerebral ischemia. J Neuropathol Exp Neurol. 1990;49(5):486–497.
243. Dietrich WD, Busto R, Valdes I, et al. Effects of normothermic versus mild hyperthermic forebrain ischemia in rats. Stroke. 1990;21(9):1318–1325.
244. Kim Y, Busto R, Dietrich WD, et al. Delayed postischemic hyperthermia in awake rats worsens the histopathological outcome of transient focal cerebral ischemia. Stroke. 1996;27(12):2274–2280; discussion 2281.
245. Zeiner A, Holzer M, Sterz F, et al. Hyperthermia after cardiac arrest is associated with an unfavorable neurologic outcome. Arch Intern Med. 2001;161(16):2007–2012.
246. Soukup J, Zauner A, Doppenberg EM, et al. The importance of brain temperature in patients after severe head injury: relationship to intracranial pressure, cerebral perfusion pressure, cerebral blood flow, and outcome. J Neurotrauma. 2002;19(5):559–571.
247. Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346(8):557–563.
248. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346(8):549–556.
249. Nolan JP, Morley PT, Hoek TL, et al. Therapeutic hypothermia after cardiac arrest. An advisory statement by the Advancement Life support Task Force of the International Liaison committee on Resuscitation. Resuscitation. 2003;57(3):231–235.
250. Shankaran S, Laptook AR, Ehrenkranz RA, et al. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N Engl J Med. 2005;353(15):1574–1584.
251. Gluckman PD, Wyatt JS, Azzopardi D, et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomised trial. Lancet. 2005;365(9460):663–670.
252. Bernard S, Buist M, Monteiro O, et al. Induced hypothermia using large volume, ice-cold intravenous fluid in comatose survivors of out-of-hospital cardiac arrest: a preliminary report. Resuscitation. 2003;56(1):9–13.
253. Haque IU, Latour MC, Zaritsky AL. Pediatric critical care community survey of knowledge and attitudes toward therapeutic hypothermia in comatose children after cardiac arrest. Pediatr Crit Care Med. 2006;7(1):7–14.
254. Schubert A. Side effects of mild hypothermia. J Neurosurg Anesthesiol. 1995;7(2):139–147.
255. Metz C, Holzschuh M, Bein T, et al. Moderate hypothermia in patients with severe head injury: cerebral and extracerebral effects. J Neurosurg. 1996;85(4):533–541.
256. National Registry of CPR (NRCPR). National Registry of CPR SAB Participant Report. American Heart Association, Dallas, TX; 2002.
257. Younger JG, Schreiner RJ, Swaniker F, et al. Extracorporeal resuscitation of cardiac arrest. Acad Emerg Med. 1999;6(7):700–707.
258. Morris MC, Wernovsky G, Nadkarni VM. Survival outcomes after extracorporeal cardiopulmonary resuscitation instituted during active chest compressions following refractory in-hospital pediatric cardiac arrest. Pediatr Crit Care Med. 2004;5(5):440–446.
259. Ronco R, King W, Donley DK, et al. Outcome and cost at a children's hospital following resuscitation for out-of-hospital cardiopulmonary arrest. Arch Pediatr Adolesc Med. 1995;149(2):210–214.
260. Schindler MB, Bohn D, Cox PN, et al. Outcome of out-of-hospital cardiac or respiratory arrest in children. N Engl J Med. 1996;335(20):1473–1479.
261. Reis AG, Nadkarni V, Perondi MB, et al. A prospective investigation into the epidemiology of in-hospital pediatric cardiopulmonary resuscitation using the international Utstein reporting style. Pediatrics. 2002;109(2):200–209.
262. Lopez-Herce J, Garcia C, Rodriguez-Nunez A, et al. Long-term outcome of paediatric cardiorespiratory arrest in Spain. Resuscitation. 2005;64(1):79–85.
263. Parra DA, Totapally BR, Zahn E, et al. Outcome of cardiopulmonary resuscitation in a pediatric cardiac intensive care unit. Crit Care Med. 2000;28(9):3296–3300.
264. Adams S, Whitlock M, Higgs R, et al. Should relatives be allowed to watch resuscitation? BMJ. 1994;308(6945):1687–1692.
265. Meyers TA, Eichhorn DJ, Guzzetta CE. Do families want to be present during CPR? A retrospective survey. J Emerg Nurs. 1998;24(5):400–405.
266. Robinson SM, Mackenzie-Ross S, Campbell Hewson GL, et al. Psychological effect of witnessed resuscitation on bereaved relatives. Lancet. 1998;352(9128):614–617.
267. Eichhorn DJ, Meyers TA, Mitchell TG, et al. Opening the doors: family presence during resuscitation. J Cardiovasc Nurs. 1996;10(4):59–70.
268. Offord RJ. Should relatives of patients with cardiac arrest be invited to be present during cardiopulmonary resuscitation? Intensive Crit Care Nurs. 1998;14(6):288–293.
269. Doyle CJ, Post H, Burney RE, et al. Family participation during resuscitation: an option. Ann Emerg Med. 1987;16(6):673–675.
270. Beckman AW, Sloan BK, Moore GP, et al. Should parents be present during emergency department procedures on children, and who should make that decision? A survey of emergency physician and nurse attitudes. Acad Emerg Med. 2002;9(2):154–158.
271. Cummins RO, Ornato JP, Thies WH, et al. Improving survival from sudden cardiac arrest: the “chain of survival” concept. A statement for health professionals from the Advanced Cardiac Life Support Subcommittee and the Emergency Cardiac Care Committee, American Heart Association. Circulation. 1991;83(5):1832–1847.
272. Herlitz J, Ekstrom L, Wennerblom B, et al. Effect of bystander initiated cardiopulmonary resuscitation on ventricular fibrillation and survival after witnessed cardiac arrest outside hospital. Br Heart J. 1994;72(5):408–412.
273. Stiell I, Nichol G, Wells G, et al. Health-related quality of life is better for cardiac arrest survivors who received citizen cardiopulmonary resuscitation. Circulation. 2003;108(16):1939–1944.
274. Locke CJ, Berg RA, Sanders AB, et al. Bystander cardiopulmonary resuscitation. Concerns about mouth-to-mouth contact. Arch Intern Med. 1995;155(9):938–943.
275. Brenner BE, Kauffman J. Reluctance of internists and medical nurses to perform mouth-to-mouth resuscitation. Arch Intern Med. 1993;153(15):1763–1769.
276. Brenner B, Stark B, Kauffman J. The reluctance of house staff to perform mouth-to-mouth resuscitation in the inpatient setting: what are the considerations? Resuscitation. 1994;28(3):185–193.
277. van Alem AP, Sanou BT, Koster RW. Interruption of cardiopulmonary resuscitation with the use of the automated external defibrillator in out-of-hospital cardiac arrest. Ann Emerg Med. 2003;42(4):449–457.
278. Hightower D, Thomas SH, Stone CK, et al. Decay in quality of closed-chest compressions over time. Ann Emerg Med. 1995;26(3):300–303.
279. Brennan RT, Braslow A. Skill mastery in public CPR classes. Am J Emerg Med. 1998;16(7):653–657.
280. Thoren AB, Axelsson A, Holmberg S, et al. Measurement of skills in cardiopulmonary resuscitation—do professionals follow given guidelines? Eur J Emerg Med. 2001;8(3):169–176.
281. Berg RA, Sanders AB, Milander M, et al. Efficacy of audio-prompted rate guidance in improving resuscitator performance of cardiopulmonary resuscitation on children. Acad Emerg Med. 1994;1(1):35–40.
282. Wik L, Thowsen J, Steen PA. An automated voice advisory manikin system for training in basic life support without an instructor. A novel approach to CPR training. Resuscitation. 2001;50(2):167–172.
283. Handley AJ, Handley SA. Improving CPR performance using an audible feedback system suitable for incorporation into an automated external defibrillator. Resuscitation. 2003;57(1):57–62.
284. Devita MA, Bellomo R, Hillman K, et al. Findings of the first consensus conference on medical emergency teams. Crit Care Med. 2006;34(9):2463–2478.
285. Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. Med J Aust. 2003;179(6):283–287.
286. Buist MD, Moore GE, Bernard SA, et al. Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study. BMJ. 2002;324(7334):387–390.
287. Hillman K, Chen J, Cretikos M, et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. Lancet. 2005;365(9477):2091–2097.