Jorge H. Castro
Juan B. Ochoa
The splanchnic organs, composed of liver, pancreas, the large and small bowel, and the gut-associated lymphoid tissue (GALT), can be a source of critical illness. These splanchnic organs also play central roles in perpetuating the multiorgan dysfunction syndrome (MODS) and failure (MOSF). As such, the critical care physician must have a significant understanding of the illnesses that arise in and relate to these organs, particularly regarding their identification and contribution to the systemic inflammatory response, to ultimately design an appropriate treatment plan and minimize the potential complications.
The complexity of the splanchnic organs is such that entire books have been dedicated to the subject. Because of its complexity, an isolated chapter will, by necessity, be only an introduction to the topic. We will describe some of the concepts that are considered most important in the relationship between gut and systemic inflammatory response syndrome (SIRS)/MODS, including the preservation of a functional intestinal barrier and the function of the GALT. The goal of this chapter, therefore, is to stimulate and prepare the reader for a more in-depth study of this area.
Basic Gastrointestinal Physiology
The gastrointestinal (GI) tract is a dual-functioning organ system that works actively in the selective absorption process; it also plays an important role in providing continuous immune surveillance and protection. The absorption of nutrients—the best-studied function of the GI tract—is essential for the processing, presentation, and delivery of all nutrients into the body. Nutrient processing is also important for maintaining a healthy gut mucosa. In addition, the gut harbors approximately 70% of all the body's immune tissue and function (1). The GALT is actively exposed to multiple antigens, and it processes these antigens and develops immunity against several environmental antigens (2,3,4).
Working in concert, the GI tract, including its mucosa and the GALT, create a sophisticated organ whose function and complexity we only partially understand. The mucosa of the GI tract is, in fact, a semipermeable membrane that acts as an intestinal barrier and is maintained by adequate blood perfusion, the secretion of mucin, and other substances such as IgA (2,5,6). Normal GI motility avoids bacterial overgrowth, and the presence of commensal organisms prevents the growth of pathogenic bacteria. Not surprisingly, alterations in all of these factors can result in disease and the development or perpetuation of SIRS or MODS (1,6,7,8).
Disease Processes That Affect the Splanchnic Organs
In critical illness, two main disease processes can lead to, or contribute to, critical illness: An inflammatory process in which an infectious agent is not initially involved, and an inflammatory process in which infection, particularly of bacterial origin, is an essential component of the disease process. However, it is important to state that in many cases, soon after the initiation of the process, which was originally without infection, bacterial contamination and invasion may play an essential role in the pathophysiology of the disease.
Inflammatory Processes Not Caused by an Infectious Agent
These include processes such as shock and ischemia–reperfusion, toxic hepatitis, or acute pancreatitis. In such disorders, the inflammatory response and activation of the immune system may proceed in the absence of infection. The clinical presentation of severe inflammation in these cases may be indistinguishable from those of diseases in which an infectious process predominates.
P.731
Inflammatory Processes in Which Infection Plays a Major Role
Disorders such as perforated appendicitis or diverticulitis with peritonitis are typical examples of this situation. In such cases, bacterial invasion of the peritoneum plays a key role in triggering the inflammatory process. The clinical presentation is classically observed as sepsis, with an acute surgical abdomen. In general, the hollow viscus is a preferred portal of entry for infection. There are, however, other forms of splanchnic organ infection not conforming to the presentation of an acute abdomen that may also be the source of a severe inflammatory response. For example, infectious pancreatitis and acute viral hepatitis can initiate the inflammatory process. A thorough review of each of these disease states is impossible in the context of this chapter; however, much is covered elsewhere in this textbook. In this chapter, we provide an outline of some of the most important and frequent processes below.
Representative Diseases of the Splanchnic Organs
Acute Pancreatitis
Acute pancreatitis is a disease process with a wide spectrum of clinical presentations and causes that can challenge any critical care physician. Only 10% to 15% of cases are severe enough to threaten patient survival, and therefore, the critical care physician tends to be involved in only the most severe cases. The most frequent causes of acute pancreatitis are gallstones and alcohol intake, constituting more than 85% of the cases (9). Other causes include hyperlipidemia, viral infections, and certain drugs such as propofol (10,11) (Tables 48.1 and 48.2).
In the intensive care unit, we should take into special consideration the association between using sedation with propofol and the presence of hypertriglyceridemia and acute pancreatitis. Devlin et al. (10) retrospectively studied 159 patients in the intensive care unit (ICU) with propofol sedation. They found that 29 (18%) patients developed hypertriglyceridemia, and among these 29 patients, 3 presented a clinical picture of acute pancreatitis. Their final recommendation was to monitor the serum triglycerides levels and pancreas enzymes after 48 hours on propofol.
Acute pancreatitis triggers the activation of endogenous enzymes such as trypsin, causing autolysis and activation of the inflammatory response. Inflammatory responses to pancreatitis can be severe enough to lead to organ failure. Bacterial seeding of the necrotic pancreas can occur, most probably through bacterial translocation from the gut, sometimes leading to the development of sepsis—one of the main causes of delayed death. It may be difficult to differentiate a severe aseptic inflammatory response to pancreatitis from a septic response due to bacterial contamination (9,12,13,14,15).
The usual initial workup for acute pancreatitis is to obtain serum amylase and lipase values and determine the severity of the disease by either APACHE II score or Ramson criteria (10) (Tables 48.3 and 48.4).
Ideally, the extension of necrosis should be determined in all cases of severe acute pancreatitis; the gold standard to make such determinations is contrast-enhanced computed tomography (CT). The CT is important for other reasons as well. For example, at times, the severity of SIRS and the early presence of shock indicates that the patient may be suffering from life-threatening complications such as major bleeding and/or hollow viscus erosion/perforation; the abdominal CT scan is useful to assess such possibilities.
|
Table 48.1 Classification System of Drug-Induced Acute Pancreatitis |
||
|
After the first 2 weeks of the disorder, the incidence of infection is increased. The patient may show a persistent inflammatory state, and can deteriorate with SIRS, sepsis, or septic shock. Although the presence of pancreatic air bubbles on abdominal CT scan suggests infection, the gold standard to rule out this possibility is CT-guided needle aspiration of the necrotic pancreatic bed (9,12,13,14,15).
Acute Mesenteric Ischemia
The splanchnic organs are perfused by three major vessels: the celiac axis, which perfuses the liver, stomach, and spleen; the superior mesenteric artery, which supplies most of the small bowel and the right side of the colon; and the inferior mesenteric artery, which supplies the left side of the colon, sigmoid, and superior portion of the rectum. Acute mesenteric ischemia is caused by several conditions including classic arterial occlusion due to atherosclerosis or embolism (frequently from the left atrium or left ventricle); low flow states due to shock, including cardiogenic shock; or mesenteric venous occlusion. Acute mesenteric ischemia frequently manifests as a devastating disease process. However, mesenteric ischemia can also present in a more subtle manner—for instance, mild abdominal distention and/or mild pain. Reperfusion of the splanchnic organs, which occurs with treatment, may also be associated with a significant and occasionally dramatic systemic inflammatory response (16,17).
|
Table 48.2 Summary of Drug-Induced Acute Pancreatitis Based on Drug Class |
|||||||||||||||
|
|||||||||||||||
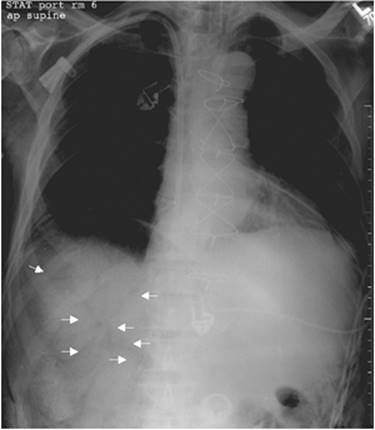
The presence of severe abdominal pain with few abdominal findings on physical exam, in any patient with risk factors, obliges the clinician to rule out this entity. Performing the examination can be made quite difficult in a sedated and ventilated patient. Hemoconcentration and/or an unexplained metabolic acidosis are indications of this disorder; occasionally, lower GI tract bleeding can be noted, or a positive stool guaiac study is obtained. Plain abdominal films are less specific, showing everything from normal findings to the demonstration of ileus, portal vein air, air in the colonic wall, or free intraperitoneal air (Figs. 48.1 and 48.2). A contrast-enhanced abdominal CT scan is useful, as it may identify the precise location of the compromised vessel (artery or vein) and extension of the damage, and signs such as portal vein air, air in the bowel wall, and complications such as free intraperitoneal air. When the patient is too unstable to be moved for a CT scan, bedside diagnostic laparotomy/laparoscopy is an option (16,17).
Extrahepatic Biliary Disease
Benign extrahepatic biliary disease (EBD) is frequently associated with varying degrees of sepsis and inflammatory response and is a common reason for admission to the ICU. Extrahepatic biliary disease includes cholecystitis and/or cholangitis. The severity of EBD increases with extremes of age and neglect related to delayed time to surgical consultation, and in patients with chronic diseases such as diabetes mellitus or those who are immunosuppressed for any reason. The main cause of EBD is the presence of gallbladder calculi.
|
Table 48.3 Ramson's Prognostic Signs of Pancreatitis Criteria for Acute Pancreatitis not Due to Gallstones |
||||||
|
||||||
Cholecystitis in the absence of calculi is also observed in the ICU, particularly in those patients who are in shock, kept without oral intake, or who received total parenteral nutrition (TPN). Acute acalculous cholecystitis may be an occult cause of sepsis and is difficult to diagnose, particularly because studies such as ultrasound lose their accuracy in the critically ill (18,19,20). Thus, the diagnosis of acalculous cholecystitis is sometimes difficult, and the intensivist must have a high index of suspicion. Usual findings are fever, hyperbilirubinemia, and right upper quadrant pain; sometimes, however, there are only signs of SIRS.
The initial study is bedside ultrasound of the right upper quadrant. Specific signs of inflammation are thickening of the gallbladder wall to greater than 3.5 mm or pericholecystic fluid. The abdominal CT scan may also be helpful in demonstrating pericholecystic fluid and pericholecystic tissue inflammation (one can obtain similar findings with ultrasound [US]), with a main disadvantage of having to transport the patient outside the ICU. On the other hand, other studies such as nuclear medicine have almost no role in the workup of the ICU patient because of the lack of specificity (18,19,20) and the need to transport the patient for this study.
|
Table 48.4 Criteria for Acute Gallstone Pancreatitis |
||||||
|
||||||
Perforation of a Hollow Viscus
Perforation of a hollow viscus with resultant intra-abdominal sepsis is a common cause for admission to the ICU. As such, the critical care physician will frequently manage these patients who present a picture of bacterial sepsis. Patients with colonic perforations may demonstrate varying degrees of septic shock. Patients with perforated peptic ulcer disease most often present initially with chemical peritonitis, which will progress to bacterial peritonitis if left untreated. Surgical management of patients with a perforated hollow viscus is an essential aspect of their care, and thus coordination between the anesthesia, surgery, and critical care teams is of great importance (21,22,23).
The combination of an acute abdomen with rapid deterioration of the patient's condition should trigger the possibility of a perforated hollow viscus. The emergent nature of the presentation will dictate the next step. Bedside plain abdomen films may, on occasion, demonstrate pneumoperitoneum; ultrasound usually does not show specific signs. The CT scan has the ability to demonstrate very small degrees of pneumoperitoneum, free fluid, duodenal wall inflammatory changes, and inflammation of surrounding organs (21).
|
|
|
Figure 48.1. This abdominal plain film shows the presence of air inside the portal vein—a classic sign for mesenteric ischemia (arrows). |
|
|
|
Figure 48.2. Note the colonic wall thickening and air bubbles in colonic wall—nonspecific signs for mesenteric ischemia (arrows). |
Clostridium difficile Colitis
The selective pressure of antibiotic use may lead to the disruption of normal fecal flora, with the emergence of resistant organisms, which can, in turn, cause disease. Best known of these organisms is Clostridium difficile, which can cause diarrheal outbreaks in health care institutions. The emergence of a hypervirulent strain of C. difficile, which produces both toxins A and B (24)—and is frequently fluoroquinolone-resistant—has been a problem of particular importance in ICUs in many countries (25). Clostridium difficile colitis can be a lethal disease, particularly if not adequately treated. There is an increased risk of developing severe C. difficile colitis in patients who are chronically ill, as well as in the elderly and immunosuppressed. Early identification and treatment are critical, and the presence of significant leukocytosis should trigger the possibility of such a diagnosis (26). The current mainstay of treatment is oral vancomycin and/or metronidazole—the latter given either intravenously or orally. Aggressive fluid resuscitation and careful monitoring of the clinical condition, along with timely surgical intervention, is important to decrease mortality. Morbidity from this disease and a significant incidence of recurrence continue to be a problem. Other adjunct treatments, including dietary manipulations, the use of probiotics and toxin-binding agents, and restoration of the colonic flora through the use of probiotics are all treatments that are being tested, though their exact role in the treatment of this disease is unclear (27). An interesting, though not appealing, idea is that of transplantation of the fecal flora, which refers to the administration of fecal flora directly to the lumen of the colon or via a nasogastric (NG) tube; preliminary results of this procedure has had promising results in small studies.
The diagnosis of C. difficile colitis may be a challenge. However, laboratory data most frequently show a leukemoid reaction on the complete blood count, and hypoalbuminemia; the most commonly used study is the toxin A and B enzyme immunoassay. If there is suspicion of megacolon, an initial abdominal radiograph—a KUB (kidney, ureters, and bladder) study—may reveal significant colonic dilatation with pneumatosis in the colonic wall. The abdominal CT scan is useful to assess colon integrity and rule out other pathologies (24).
The Abdomen As an “Unknown Source of Sepsis”
Evaluation of the abdomen as the source of sepsis in the ICU patient is difficult. Clinical examination in a neurologically intact patient remains the gold standard used to rule out an acute surgical abdomen and the identification of the abdomen as a source of sepsis. This is not the case in many critically ill patients in whom neurologic impairment due to the primary disease, or resultant from sedation, abrogates good communication with the patient and a dependable clinical examination. In fact, performing a good clinical examination was not possible in 43% to 69% of patients in the ICU (28). Particularly difficult are those who have had recent previous abdominal surgery, and in whom an intra-abdominal septic complication could be a potential cause of critical illness.
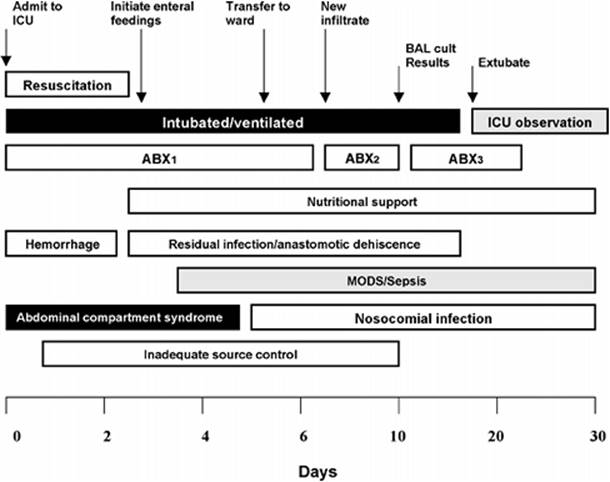
How is one to open the “black box” of the abdomen and identify an occult source of sepsis? Several conditions such as pancreatitis and mesenteric ischemia could develop during the intensive care unit admission or may be the primary reason for admission. The diagnostic approach in these patients is dictated by several factors, including the severity of the critical illness, the availability of different diagnostic tools, and the availability of specialized consultants (Fig. 48.3). In patients with severe hemodynamic instability and/or marginal ventilatory status, transport to radiologic suites or other diagnostic facilities may not be possible; also, portable CT scanners are often not available. Therefore, it is important for the critical care physician to identify the available tools that can assist him or her in the timely diagnosis and management of occult abdominal sepsis.
|
|
|
Figure 48.3. Scheme showing when, during the course of an intensive care unit admission, intra-abdominal problems are more likely to be seen, especially after abdominal or interventional procedures. ABX, antibiotics; BAL cult, bronchoalveolar lavage culture; ICU, intensive care unit; MODS, multiorgan dysfunction syndrome. (From Crandakk M, West MA. Evaluation of the abdomen in the critically ill patient: opening the black box. Curr Opin Crit Care. 2006;12:333–339, with permission.) |
The use of radiologic studies such as CT scan, ultrasound, and nuclear medicine imaging require careful evaluation of the risks associated with the specific study versus the benefit from the information obtained. It is important to emphasize that none of the imaging studies used to diagnose an acute intra-abdominal process is risk-free. For example, studies such as abdominal CT scanning require transport outside of the ICU, and the use of contrast material can produce serious toxicity, such as acute renal failure with intravenous (IV) contrast media administration, as well as discomfort and pain. The information yielded by any of the studies may be poor or lead to misinterpretation, thereby increasing morbidity; thus, the authors discourage the use of diagnostic tests in a “fishing expedition” mode. The studies requested must be done to answer a specific question or questions and the results provided by the study. Furthermore, the risks must be offset by the benefits accruing to the patient, which is not always a simple calculation.
Occasionally, the intensivist appeals to the surgeon to perform an exploratory laparotomy as a means to diagnose and treat intra-abdominal illness. Blind exploratory laparotomies, however, have yielded uniformly poor results, generally not identifying the source of infection, while significantly increasing morbidity or mortality (28). Other less aggressive modes of surgical diagnostic interventions have, therefore, been designed, including diagnostic peritoneal lavage (DPL), paracentesis, and bedside laparoscopy.
Abdominal Compartment Syndrome
Increased intra-abdominal pressures compromising blood flow to splanchnic organs have been described in an increased percentage of patients in the ICU. In a recent article, for example, Malbrain et al., from the European Community (29), analyzed 265 consecutive patients in the ICU, measuring intra-abdominal pressures via transduction of the urinary bladder. This work demonstrated that nonsurvivors tended to have higher intra-abdominal pressures. Furthermore, patients with prior elevated intra-abdominal pressures exhibited increased sepsis-related organ failure assessment (SOFA) scores.
Determining when abdominal decompression should be done remains controversial and is partially subjective. For some, intra-abdominal hypertension (IAH) is defined as a pressure greater than 20 mm Hg in the presence of at least one organ failure. In these cases, opening the abdomen should be considered and should be viewed as a therapeutic maneuver to improve splanchnic organ perfusion. Demonstrating that surgical therapy improves outcome is, however, difficult. Nonetheless, it is logical that increasing organ perfusion should improve physiologic function, or at least not worsen the outcome.
Bacterial Translocation from the Gut
Maintenance of the gut mucosal physiologic barrier prevents the passage of bacteria—or bacterial products such as endotoxin—into the systemic circulation. Once the gut undergoes a predisposing condition, such as an ischemia–reperfusion insult, bacteria and endotoxins can traverse the intestinal barrier and seed distant organs such as mesenteric lymph nodes (MLNs), solid organs, and the bloodstream; this is termed bacterial translocation. Several studies have added to the evidence linking bacterial translocation and the systemic inflammatory response (1,2,3,4). Bacterial translocation (BT) is associated with postoperative sepsis in up to 14%, as demonstrated by MacFie et al. (3). Prevention of bacterial translocation is essential, and is accomplished by careful maintenance of organ perfusion, judicious use of antibiotics, and avoidance of excessive IV fluids. Perhaps the most important preventative factor is the early institution of enteral nutrition support.
Special Concerns With Ileus
Normal gastrointestinal motility permits a downstream (aboral) progression of secreted fluids and food through the gastrointestinal tract. It also prevents bacterial overgrowth and provides the adequate contact of nutrients with the gut mucosa, thereby allowing digestion and absorption. Loss of coordinated propulsive motor impulses may result in decreased digestion and absorption of food and liquids, gastrointestinal intolerance, and the lack of passage of flatus or stool; this is called ileus. Ileus is therefore a functional intestinal obstruction in the absence of mechanical evidence of obstruction.
Ileus, in its worse clinical presentation, is a manifestation of organ (gastrointestinal) dysfunction or failure. Ileus can result in abdominal compartment syndrome, severe electrolytic disturbances, and bacterial overgrowth. Furthermore, the presence of ileus precludes successful enteral nutritional interventions. For these reasons, adequate identification of ileus is an essential aspect of care of the critical care physician.
The diagnosis of ileus is often inaccurate and is based on significant preconceptions that are frequently erroneous. For example, it is often believed that surgical intervention on the gastrointestinal tract results in ileus, and that, postoperatively, this patient population should be kept without oral or enteral intake. Similar misconceptions are often observed with artificially established amounts of gastric residuals or nasogastric outputs. Paradoxically, multiple patients are often kept without enteral intake, which only exacerbates gastrointestinal dysfunction and provides an inadequate and/or inappropriate diagnosis of ileus.
Ileus has to be carefully identified by radiographs and a thorough clinical assessment. Careful hydration and restoration of splanchnic blood flow through adequate resuscitation are essential. The judicious use of enteral nutritional support and avoiding prolonged time periods without enteral intake are essential to the prevention and treatment of ileus. Furthermore, the careful treatment of the cause of an ileus, such as sepsis, will often result in the spontaneous resolution of the gastrointestinal process. Maintenance of fluid and electrolyte balance are also important.
When to Feed?
Early enteral nutrition (EEN) has proven to be beneficial, and should be started as soon as possible in the ICU patient, as there are multiple studies demonstrating the benefits of enteral nutrition. For example, Moore et al. (30) found that starting early enteral feeding significantly decreased the risk of infections (p <0.05). In contrast, the use of total parenteral nutrition (TPN)—particularly when selected instead of EEN—was associated with significant harm when performed by inexperienced personnel and/or if there was inadequate patient selection.
The mechanisms that explain why EEN is superior to TPN are only partially understood. Routinely, patients on TPN achieve higher caloric goals than on EEN, but despite this practice, patients routinely do better in the absence of TPN. Thus, the benefits of EEN are not linked to the number of calories received by the patient. Starvation is associated with increased mucosal permeability along with increased expression of ICAM-1, favoring the migration of PMNs to the intestine wall compared with enteral-fed animals (31). Another interesting experiment showed that adding bombesin, an analogue of gastrin-releasing peptide, can recover the GALT in mice on TPN and, indeed, preserve the immune response to infections (32). Kudsk (33) reviewed the literature regarding EEN, finding fewer infections and better outcomes when such therapy was used. In addition, Andrad et al. (34) studied rats receiving either standard TPN or glutamine-enriched TPN. They found less bacterial translocation in the group on glutamine-enriched TPN, suggesting that glutamine, an amino acid, improves the response to antigens and increases the IgA levels, as reported previously (35). Other authors have reported that EEN prevents GALT atrophy and the development of SIRS/MOD (36,37,38).
Summary
Splanchnic organs continue to be a challenge for intensivists. Splanchnic organs can both be a source of disease and perpetuate existing problems. Maintenance of normal splanchnic organ function is essential for the survival of the patient. Gut trophism and immune function is better preserved by enteral/oral nutrition. Therefore, EEN should be the standard of care in trauma services.
References
1. Schmidt H, Martindale R. The gastrointestinal tract in critical illness. Curr Opin Clin Nutr Metab Care. 2001;4:547–551.
2. Achenson DWK. Mucosal immune responses. Best Pract Res Clin Gastroenterol. 2004;18:387–404.
3. MacFie J, Reddy BS, Gatt M, et al. Bacterial translocation studied in 927 patients over 13 years. Br J Surg. 2006;93:87–93.
4. Moore F. The role of the gastrointestinal tract in postinjury multiple organ failure. Am J Surg. 1999;178:449–453.
5. Moore E, Moore FA, Franciose RJ, et al. The postischemic gut serves as a priming bed for circulating neutrophils that provoke multiple organ failure. J Trauma. 1994;37:881–887.
6. Leaphart CL, Tepas III JJ. The gut is a motor of organ dysfunction. Surgery. 2007;141:563–569.
7. Laughlin RS, Musch MW, Hollbrook CJ, et al. The key role of Pseudomonas aeruginosa PA-I lectin on experimental gut-derived sepsis. Ann Surg. 2000;232:133–142.
8. Reinhart K, Bloos F, Brunkhorst. Pathophysiology of sepsis and multiple organ dysfunction. In: Fink M, Abraham E, Vincent JL, et al., eds. Textbook of Critical Care. 5th ed. Philadelphia, PA: Elsevier Saunders; 2005:1257.
9. Badalov, N, Baradarian, R, Iswara, K, et al. Drug-induced acute pancreatitis: an evidence-based review. Clin Gastroenterol Hepatol. 2007;5:648–661.
10. Devlin JW, Lau AK, Tanios MA. Propofol-associated hypertriglyceridemia and pancreatitis in the intensive care unit: an analysis of frequency and risk factors. Pharmacotherapy. 2005;10:1348–1352.
11. Beger HG, Rau B, Mayer J, et al: Natural course of acute pancreatitis. World J Surg. 1997;21:130–135.
12. Zhao X, Anderson R, Wang X, et al. Acute pancreatitis-associated lung injury: pathophysiological mechanisms and potential future therapies. Scand J Gastroenterol. 2002;37:1351–1358.
13. Mann DV, Hershman MJ, Hittinger R, et al. Multicenter audit of death from acute pancreatitis. Br J Surg. 1994;81:890–893.
14. Hartwig W, Werner J, Uhl W, et al. Management of infection in acute pancreatitis. J Hepatobiliary Pancreat Surg. 2002;9:423–428.
15. Ramson JHC. Etiological and prognostic factors in human acute pancreatitis: a review. Am J Gastroenterol. 1982;77:633–638.
16. Haglund U. Gut ischaemia. Gut. 1994;35:S73–76.
17. Brandt LJ, Boley SJ. AGA technical review on intestinal ischemia. American Gastrointestinal Association. Gastroenterology. 2000;118:954–968.
18. Glenn F, Becker CG. Acute acalculous cholecystitis: an increasing entity. Ann Surg. 1982;195:131–136.
19. Boland G, Lee MJ, Mueller PR. Acute cholecystitis in the intensive care unit. New Horiz. 1993;1:246–260.
20. Ryu JK, Ryu KH, Kim KH. Clinical features of acute acalculous cholecystitis. J Clin Gastroenterol. 2003;36:166–169.
21. Solomkin JS, Wittman DW, West MA, et al. Intraabdominal infections. In Schwartz SI, Shires GT, Spencer FC, et al., eds. Principles of Surgery, 7th ed. New York, NY: McGraw-Hill; 1999:1515–1550.
22. Anaya DA, Nathens AB. Risk factors for severe sepsis in secondary peritonitis. Surg Infect (Larchmt). 2003;4:355–362.
23. Fry DE, Pearlstein DE, Fulton RL, et al. Multiple system organ failure: the role of uncontrolled infection. Arch Surg. 1980;115:136–140.
24. Fekety R, Shah AB: Diagnosis and treatment of Clostridium difficile colitis. JAMA. 1993;269:71.
25. Razavi B, Apisarnthanarak A, Mondy LM. Clostridium difficile: emergence of hypervirulence and fluoroquinolone resistance. Infection. 2007;5:300–307.
26. Wanahita A, Goldsmith EA, Musher DM. Conditions associated with leukocytosis in a tertiary care hospital with particular attention to the role of infection caused by Clostridium difficile. Clin Infect Dis. 2002;34:1585–1592.
27. Miller MA. Clinical management of Clostridium difficile-associated disease. Clin Infect Dis. 2007;45:S122–S128.
28. Crandall M, West MA. Evaluation of the abdomen in the critically ill patient: opening the black box. Curr Opin Crit Care. 2006;12:333–339.
29. Malbrain M, Chiumello D, Pelosi P, et al. Incidence and prognosis of intraabdominal hypertension in a mixed population of critically ill patients: a multiple-center epidemiological study. Crit Care Med. 2005;33:315–322.
30. Moore FA, Feliciano DV, Andrassy RJ, et al. Early enteral feeding, compared with parenteral, reduces postoperative septic complications. The results of a meta-analysis. Ann Surg. 1992;216:172–183.
31. Fukatsu K, Zarzaur BL, Johnson CD, et al. Enteral nutrition prevents remote organ injury and death after a gut ischemic insult. Ann Surg. 2001;233:660–668.
32. DeWitt RC, Wu Y, Renegar KB, et al. Bombesin recovers gut-associated lymphoid tissue and preserves immunity to bacterial pneumonia in mice receiving total parenteral nutrition. Ann Surg. 2000;231:1–8.
33. Kudsk KA. Early enteral nutrition in surgical patients. Nutrition. 1998;14:541–544.
34. Andrade M, Santos D, Fernandez S, et al. Prevention of bacterial translocation using glutamine: a new strategy of investigation. Nutrition. 2006;22:419–424.
35. Sawai T, Goldstone N, Drongowski RA, et al. Effect of secretory immunoglobulin A on bacterial translocation in an enterocyte-lymphocyte co-culture model. Pediatr Surg Int. 2001;17:275–279.
36. Avenell A. Glutamine in critical care: current evidence from systematic reviews. Proc Nutr Soc. 2006;65:236–241.
37. Wildhaber B, Yang H, Spencer A, et al. Lack of enteral nutrition. Effects on the immune system. J Surg Res. 2005;123:8–16.
38. MacFie J. Enteral versus parenteral nutrition: the significance of bacterial translocation and gut-barrier function. Nutrition. 2000;16:606–611.