Stephanie A. Savage
Timothy C. Fabian
The practice of surgery inevitably carries the risk of postoperative complications and difficult therapeutic choices. Some of the most vexing operative dilemmas result from managing a difficult postoperative abdomen. Routine intra-abdominal therapies will result in adhesion formation, which may plague the patient with recurrent episodes of abdominal pain and partial or complete bowel obstruction. Enterocutaneous, intra-abdominal, or pancreatic fistulas may result from the natural progression of intra-abdominal pathology or may be the sequelae of invasive procedures. Abdominal catastrophes may result in a compartment syndrome mandating aggressive management decisions including temporary abdominal closures and planned ventral hernias. Less common issues, including radiation enteritis and short bowel syndrome, may significantly impact lifestyle and health, requiring surgical attention.
In this chapter, we will address many of these difficult postoperative issues. Our discussion will include etiology, diagnosis, and therapeutic approaches. The core principles of careful surgical technique and meticulous patient management, including wound care, nutritional management, and timing of recurrent interventions, are key in treating these obstacles.
Adhesions
Intra-abdominal adhesions are an unavoidable consequence of operative therapy. Intra-abdominal adhesions are the primary cause for postoperative bowel obstruction, accounting for approximately 75% of cases (1). Adhesions intrinsically play a crucial role in postoperative healing. Formation of adhesive tissue protects an anastomosis and prevents leaks, in addition to assisting in the body's attempt to isolate intra-abdominal catastrophes like abscesses. When adhesive bands become too dense, kink, or encompass loops of bowel, they may result in negative consequences such as bowel obstruction and persistent abdominal pain. In this chapter, we will discuss the development of adhesions, their natural history, and methods of prevention.
Adhesion formation occurs in the course of repairing an injury site, anastomosis, or incision. Within the first 48 to 72 hours of injury, macrophages converge to form a protective layer over the injured tissue. These macrophages further differentiate into mesothelial cells, while additional fibroblasts and mesothelial cells are recruited from nearby locales. These cell populations complete the initial stages of healing over a period of 7 to 10 days (2,3). Ultimately, these healing cell populations will not only continue the process of restoring tissue integrity but may form unnatural connections. Adhesive connections may occur between loops of bowel, intra-abdominal structures and the abdominal wall, and between the pelvis and nearby structures (bowel, gynecologic organs, etc.) resulting in intra-abdominal pathology and patient morbidity.
Most (94%–98%) of abdominal adhesions are acquired, either from operative therapy or via inflammatory processes (i.e., Crohn's disease, cancer, etc.). The remaining 2% to 6% of adhesions are congenital and largely consist of Ladd bands. In the reoperative abdomen, adhesions are present in 30% to 40% of patients. The most frequent morbidity in those with postoperative adhesions is small bowel obstruction, which accounts for 12% to 17% of hospital admissions following previous abdominal surgery. One quarter of these admissions occur within the first year following surgery, and 2% to 5% of small bowel obstructions due to adhesions will require operative adhesiolysis (2). The degree of morbidity related to adhesion formation is profoundly affected by the type of surgery performed. Laparoscopic surgeries have been shown to have a 15% adhesion rate as opposed to open laparotomies, in which 50% result in adhesion formation. Adhesion formation tends to follow predictable patterns. Adhesions form more commonly following surgery to the small and large bowel than with other intra-abdominal organs, especially in surgeries involving bowel distal to the transverse colon or involving gynecologic organs (1). The areas most frequently affected are the under surface of the midline incision and the operative site, for example at an anastomosis. Due to its tendency to migrate to regions of inflammation, the omentum is the most frequently involved organ (57%). Small and large bowel adhesions continue to result in the highest morbidity (4).
The cost of adhesion-related disease, both regarding morbidity and monetarily, has resulted in extensive research focused on developing methods to avoid adhesion formation. Adhesions result from trauma to tissues, relative ischemia, infection within the abdominal cavity, inflammatory processes, or by the presence of foreign bodies such as suture, talc from gloves, and lint from sponges. To minimize adhesions, principles of good surgical technique are the best defense. Gentle tissue handling with strict hemostasis and minimization of intraperitoneal trauma are core principles. In addition, frequent irrigation to dilute or to remove contaminants and the use of small, nonreactive suture material will diminish the contribution to adhesiogenesis. Raw surfaces or anastomoses should be protected by autologous tissue, either with a tongue of omentum or via mobilized local tissue flaps. Perhaps the most effective method of preventing serious adhesions is via the use of the omentum. As is well known, the omentum is key to protecting areas of inflammation and infection within the abdomen. In a similar manner, the omentum may be used to wrap anastomoses or to protect abdominal contents from a healing midline incision. Unfortunately, the omentum is often too limited by prior inflammatory processes or surgery to be of use.
Barriers to Adhesiogenesis
Despite meticulous technique and conscientious efforts to prevent adhesions, they will continue to form with attendant postoperative morbidity and mortality. Research efforts have focused on developing materials to minimize the occurrence and severity of adhesions. The most common method of decreasing the number and strength of adhesions is with one of a variety of barrier materials. Seprafilm (Seprafilm Adhesion Barrier, Genzyme Corporation, Cambridge, MA) is an FDA-approved material composed of hyaluronic acid and carboxymethylcellulose. Applied to regions at risk for adhesions, it forms a deposit that acts as a mechanical barrier to adhesion formation. It is eventually reabsorbed by the body after 7 to 10 days. One large study demonstrated no difference in rates of small bowel obstruction with Seprafilm; however, the need for operative therapy to treat adhesions was significantly reduced (1). Of note, Seprafilm should not be used to wrap anastomoses to decrease adhesions at these sites, as this has resulted in higher rates of fistula formation (1). Interceed (Gynecare Interceed, Johnson & Johnson, New Jersey) is an older option that is a mechanical barrier designed to be placed over injured surfaces and operative sites. It is composed of oxidized regenerated meshlike cellulose; data have been mixed on its effectiveness. Although some studies have demonstrated that Interceed is safe and effective in reducing adhesions, other studies have shown no clinical benefit from its use (4). Additionally, it requires a completely hemostatic field, and the region in question must be completely covered for effective results, not always practical especially in laparoscopic surgery. Other methods to decrease adhesion formation have been shown to be less effective in adhesion prevention and are not used commonly in clinical practice. Gore-Tex Surgical Membrane (W.L. Gore and Associates, Flagstaff, AZ), a thin PTFE (polytetrafluoroethylene) membrane that prevents cellular penetration, must be secured in place and removed at a later date. This method is cumbersome, has not shown significant clinical benefit in preventing adhesions, and is not commonly used. Streptokinase infusion has shown no benefit in reducing adhesions. The use of tissue plasminogen activator to break down adhesions has shown some promise in animal studies but has not been proven in humans to date (4,5). These latter methods are of interest, either historically or in a research perspective, but are not commonly used in clinical practice.
Regardless of which product is ultimately chosen, the ideal barrier would be nonreactive in vivo, would be active during the key healing stages, and then be reabsorbed by the body when no longer needed. Locales that remain prime candidates for adhesion barriers include around temporary stomas, around the Hartman pouch after colectomy, beneath the midline incision, and in the pelvis following surgery in that region, especially in patients prone to inflammation. Research interest in this area remains high as adhesion-related morbidity continues to plague surgical patients.
Fistulas
A fistula is an abnormal communication between two spaces. In the abdomen, varieties of fistulas differ tremendously and include such types as pancreatic fistulas, biliary fistulas, fistulas between two intra-abdominal organs (i.e., colovesical fistulas), and enterocutaneous fistulas. The natural history of a fistula begins as a leak from bowel or other intra-abdominal organ. The ultimate type of fistula depends on whether the leak is uncontrolled, partially controlled, or well controlled. An uncontrolled leak will result in peritonitis, which immediately results in surgical exploration and correction. A partially controlled leak may result in an intra-abdominal abscess, which will require definitive therapy. Controlled leaks result in fistulas, and the most dreaded of these is the enterocutaneous fistula. Management of fistulas can be a long-term challenge for surgeon and patient.
An enterocutaneous fistula is an abnormal communication between lumen of bowel and the skin. Fistulas are postoperative complications in 71% to 90% of cases, though they may occur spontaneously (2,6). Spontaneous causes of fistulas are uncommon but may include malignancy, inflammatory processes such as Crohn's disease, or vascular insufficiency, as seen in radiation enteritis. The iatrogenic fistula is the most common and presents a difficult management problem. Iatrogenic fistulas may result from inadvertent enterotomies, intra-abdominal infections, direct injury or bowel desiccation in the open abdomen, misplaced stitches, or anastomotic breakdown. Impaired tissue perfusion from hypotension or vascular disease may predispose to this complication, as will infections, steroids, and malnutrition.
An enterocutaneous fistula typically presents as discolored, watery drainage from the midline incision. A seeming wound infection opened at bedside will result in copious drainage of discolored, watery material or frank succus. Passage of gas from the midline wound is diagnostic of an enterocutaneous fistula. Patients will usually demonstrate signs of advancing infection including increasing temperature, white blood cell count, and persistent ileus. In less common cases, patients may develop profound shock due to electrolyte imbalances and sepsis. In these cases, emergent re-exploration is necessary. However, if the patient presents with drainage or an obvious fistula but is hemodynamically stable, conservative management is warranted, at least in the short term.
Conservative Management of the Enterocutaneous Fistula
Management is predicated on controlling output, managing electrolyte fluxes and nutritional deficiencies, and maximizing the potential for spontaneous closure (Fig. 77.1). In the immediate care of the patient, aggressive fluid resuscitation and close monitoring of electrolyte balance are mandatory to maintain stability. If the patient remains stable without the need for emergent operative intervention, nutritional replacement should begin immediately. This patient population is exceptionally prone to malnutrition from protein losses, increased metabolic demands, and limited or no oral intake. Parenteral nutrition is nearly mandatory to provide early and aggressive nutritional repletion, to allow close management of electrolyte and protein balances, and to decrease volume transit past the fistula in the gastrointestinal tract. Perhaps a greater challenge in this patient population is control of fistula output. Enteric contents are extremely caustic to the skin and surrounding tissues. An immediate goal in caring for patients with fistulas is to create some method to isolate enteric contents from the skin. For a simple enterocutaneous fistula, a stoma appliance may be all that is needed. However, many fistulas present in open wound beds, including on granulating abdomens. These tissue fields are not amenable to the placement of a simple stoma appliance. In these situations, a close association between the surgeon, patient, and wound care nurse/enterostomal therapist is mandatory to control fistula output. Once initial control is achieved, it may be possible to close fistulas surgically or to skin graft the region. These surgical options will be discussed in more detail later in this section
|
|
|
Figure 77.1. Management strategy for managing enterocutaneous fistulas. |
Spontaneous Closure
The goal of conservative therapy is to achieve spontaneous closure of the fistula. Spontaneous closure is dependent largely on inherent characteristics of the fistula. Most fistulas that close without intervention will do so in the first 3 to 6 weeks after appearance. Fistulas with long tracts and narrow mouths are most likely to resolve independently. Additionally, low-output fistulas, defined as having an output less than 500 mL per day, have a higher likelihood of closure than high-output fistulas. A fistula that is not closed by 3 months is unlikely to close without surgical therapy. Additionally, many patient factors have been associated with failure of the fistula to close spontaneously. Factors that will virtually ensure patency of the fistula include the presence of a foreign body in the fistula tract, close association between the fistula and an abscess, association with a malignancy, distal bowel obstruction leading to increased pressure and transit through the fistulous tract, epithelialization of the tract, and a short neck with wide fistula mouth. As noted, long-standing fistulas with high outputs are unlikely to close spontaneously.
The patient and surgeon are not completely at the mercy of physiology and chance while awaiting spontaneous closure. At least in the short term, parenteral nutrition is pursued to decrease the volume transiting the gastrointestinal tract and through the fistula. A positive nitrogen balance and a transferrin level greater than 200 mg/dL are also associated with successful closure (7). The use of octreotide or other somatostatin analogue (100 µg intravenously every 8 hours) may decrease secretion in the gastrointestinal tract as well. Somatostatin inhibits the secretion of most gastrointestinal hormones and enhances fluid and electrolyte absorption, thereby decreasing intraluminal volume and potentially decreasing fistula output. Despite the theoretical benefits of somatostatin use, clinical studies have revealed mixed results on effectiveness. Although some studies have demonstrated a decreased fistula output and higher rate of spontaneous closure, an equivalent literature reveals no statistical difference in output or closure rates (8). As side effects are relatively mild, including gastrointestinal discomfort and increased biliary sludge, we recommend trying a somatostatin analogue in conjunction with other conservative therapies while waiting for a fistula to close spontaneously. However, somatostatin analogues should not be relied on as a primary therapy to close fistulas.
Surgical Therapy for Enterocutaneous Fistulas
If after approximately 3 months a fistula has failed to resolve, the likelihood of closure without operative intervention is poor. The first step in surgical closure is defining the fistula. The best method of defining a fistula tract is via fistulogram. In the standard method, Gastrografin is injected into the tract and fluoroscopy is used to follow the progress of the contrast. A fistulogram is useful to define the length of the tract, tortuosity, tract diameter, and which segment of the gastrointestinal tract is involved. An alternative method described in the litrature supports the use of hydrogen peroxide–enhanced ultrasound. The fistula is injected with hydrogen peroxide and ultrasound is used to define the tract. This method has no associated radiation, and ultrasound allows inspection of other intra-abdominal organs. A computed tomography (CT) scan may also be helpful in defining intra-abdominal abscesses, malignancy, and hernias (9).
In addition to defining the nature of the fistula, it is imperative that the patient's nutrition be maximized at the time of repair. Attention should be paid to control of fistula output, as healthy skin at the time of operation will improve the success of abdominal wall reconstruction (8). Essentially, by delaying operative repair until all criteria are met (nutrition, fistula definition, wound care), the morbidity and mortality may be decreased from 50% mortality and 50% recurrence in early surgeries to 94% successful closure and a 4% mortality rate with careful planning and delayed surgery (2,10).
Laparotomy with formal surgical repair is typically not the first surgery performed for these patients. A particular challenge for surgeons attempting to address enterocutaneous fistulas operatively is the condition of intra-abdominal adhesions. Extensive, dense adhesions may make access to the fistula very difficult, and there is a real risk of multiple enterotomies in approaching the segment involved in fistulization. A common initial attempt is to oversew the fistula primarily. Indeed, this technique may even be attempted at formal laparotomy. Although it may be appealing due to simplicity and avoidance of an anastomosis, it has a dismal failure rate and often results in a larger fistula. Simply oversewing fistulas should be avoided whenever possible. The preferred method for definitive surgical therapy remains complete lysis of intra-abdominal adhesions and resection of the involved segment. With this method, the diseased portion of bowel is removed and the anastomosis is performed between two healthy segments of intestine. The complete lysis of adhesions allows careful inspection of small bowel to rule out downstream obstruction or other pathology. Although potentially time consuming and technically demanding, this approach provides the highest likelihood of recovery without recurrent fistulization.
Enterocutaneous fistulas are unfortunately common in the open, granulating abdomen. These fistulas are an especially challenging management problem as it is difficult to control output on the granulating abdominal bed. A superior option for the patient with a fistula in the face of the granulating, open abdomen is the split-thickness skin graft. Although the skin graft rarely results in fistula closure, the adherence of the graft to the remainder of the granulation bed is excellent. The skin graft will decrease the metabolic demands of a granulating abdomen in an already stressed body and provide a good base for appliances placed for control of fistula output. For patients who may not tolerate an extensive repeat laparotomy, local mobilization of the fistula tract may allow for definitive closure. The fistula and the bowel are mobilized circumferentially proximally and distally by local dissection. The fistula portion is resected and closed, and the entire abdomen is covered with a split-thickness skin graft. Advocates claim a 56% success rate for this technique, and it may indeed be a better choice for some patients (2). In general, the split-thickness skin graft, with or without fistula closure, is more successful in low-output fistulas. High-output fistulas will stress a fistula repair leading to recurrent fistulization. Additionally, high fistula outputs will interfere with adherence of the grafted skin and ultimately digest the skin graft. Therefore, as with most procedures, careful patient selection will improve the success rate.
The Pancreatic Fistula
The pancreatic fistula is of an entirely different nature. In surgical patients, these fistulas most often result from trauma or iatrogenic injury, though a small percentage will be the result of pancreatitis. The cardinal principles of management are diagnosis of the fistula and wide drainage. A pancreatic fistula may drain from 100 to 1,000 mL of fluid per day. The resulting pancreatic ascites may cause abdominal pain, fevers, and a plethora of vague symptoms including abdominal bloating, hiccups, intolerance to oral intake, and abscess. Pancreatic fluid contains a large amount of bicarbonate compared to plasma (70–90 mEq/L), and inadequate replacement of bicarbonate may lead to nonanion gap metabolic acidosis. All patients respond differently to a pancreatic leak, and whereas some may present in profound shock, other patients may tolerate large-output pancreatic fistulas with few signs or symptoms. The source of this variability in clinical presentation is poorly understood but is likely due to the degree of enzymatic activation of the leaking fluid. The most common method of diagnosis is by CT scan. If the patient is of reasonable body habitus and transport is hazardous, an ultrasound may provide equivalent information.
For most patients, the initial treatment for a pancreatic fistula is simply drainage. In the modern era, interventional radiology is invaluable in placing these drains. However, if at initial operation there is concern for postoperative leak, wide drainage with a closed-system drain should be established before closing the patient's abdomen. Wide drainage of pancreatic secretions should allow time for the patient to stabilize and prevent damage to other abdominal organs. Frequently, patience to allow long-term drainage to resolve will permit spontaneous closure of the pancreatic fistula. In addition to drains, adjuncts such as total parenteral nutrition and octreotide may be helpful in decreasing secretory stimulation to the pancreas. A multiseries review demonstrated that the octreotide group (administered 100 µg subcutaneously every 8 hours begun immediately after procedures deemed at high risk for pancreatic fistulas) had reduced fistula outputs, lower serum amylase and lipase levels, and an earlier return of positive nitrogen balance than in control groups (8). As in many areas of research, there is an opposing literature demonstrating no statistically significant improvement in patient outcomes with octreotide therapy. However, it is reasonable to pursue this therapy for a time-limited course (approximately 1 week) to improve chances of nonoperative resolution.
Conservative management with drains is generally pursued for up to 6 months and has a success rate of upto 97% in some studies (11). Depending on the cause of the fistula, intervention may be indicated on an earlier basis. If drainage fails to resolve the fistula, an imaging study should be pursued to define the duct and to determine if an obstructive process is mandating fistula patency. Although both magnetic resonance cholangiopancreatography (MRCP) and endoscopic retrograde cholangiopancreatography (ERCP) may provide equivalent information, ERCP is preferred. ERCP allows the opportunity to identify pathology of the pancreatic duct and also allows the opportunity to intervene. Stenting of a proximal obstruction may be adequate to allow prograde drainage of pancreatic secretions and closure of the fistula, thereby avoiding surgical therapy (12). When all less invasive therapies fail, however, exploratory laparotomy remains the gold standard for definitive therapy. Options at laparotomy depend on the level of the injury. Primary duct repair is unlikely in most circumstances. Rather, a fistula resulting from the distal duct (perhaps secondary to a splenectomy) is well treated by distal pancreatectomy. If the leaking duct is sufficiently large, as is seen in relation to a ductal obstruction, a pancreaticojejunostomy may be performed to allow for a low-resistance drainage pathway. Pancreatic fistulas involving the proximal duct are most often iatrogenic or related to trauma and are troublesome to deal with, in light of other major structures in the region. For these patients, a pancreaticoduodenectomy (Whipple procedure) will resect the leaking portion of pancreas and allow reconstruction. The Whipple procedure should be entertained only in patients with good physiologic reserve. As noted, an attempt at conservative therapy and complete preoperative imaging and optimization are mandatory as these procedures are a major commitment for surgeon and patient. Despite the wealth of surgical options, most pancreatic fistulas will resolve with appropriate drainage, and thus, surgical correction is an end-stage option for correction of the fistula (11).
Abdominal Compartment Syndrome
Abdominal compartment syndrome has historically been a source of significant patient morbidity and mortality. First described in 1984, abdominal compartment syndrome was the result of an intra-abdominal catastrophe (ruptured abdominal aortic aneurysm) resulting in elevated pressure and multiple highly morbid sequelae (13). More recently, secondary abdominal compartment syndrome has resulted from massive resuscitations required by major trauma, burns, and pancreatitis. Regardless of the source of the compartment syndrome, those requiring decompressive laparotomy have a mortality rate of 19% to 33% (14). Occurrence of abdominal compartment syndrome has been lessened somewhat within the last decade due to increased recognition of the phenomenon and prophylactic use of the open abdomen technique. In operative cases requiring large-volume resuscitations, the abdomen is frequently left open postoperatively until edema decreases enough to allow tension-free primary closure. In this way, compartment syndrome and its sequelae are avoided. In the following section, diagnosis and management of abdominal compartment syndrome will be addressed, including methods to care for the open abdomen.
Since its first description in the 1980s, abdominal compartment syndrome has become an increasingly recognized clinical entity. Although classically described as a primary entity, in current surgical therapy it is usually seen following a massive fluid resuscitation from trauma, burns, intraoperative resuscitation, pancreatitis, or sepsis. Capillary leak occurs secondary to sepsis or reperfusion injury in the splanchnic circulation and results in massive interstitial edema. As the abdomen is a limited potential space, increasing interstitial edema and free fluid in the abdomen result in increased intra-abdominal pressure, which is transmitted to organs in both the thorax and abdomen. The physiologic effects range from cardiovascular to pulmonary to renal. Compression of the inferior vena cava by abdominal contents and fluid results in decreased preload and a subsequent decrease in cardiac output. This ultimately leads to increased systemic vascular resistance and decreased stroke volume. Clinically, patients will become increasingly tachycardic and hypotensive. Increased abdominal volume also places pressure on the diaphragm, limiting intrathoracic space. This results in increasing peak ventilatory pressures (greater than 30–35 mm Hg) and decreased ventilation with hypercapnia and hypoxemia. Compression of the ureters and bladder, as well as renal vein compression, leads to diminished urine output and renal injury, as well as elevated bladder pressures (greater than 25–30 mm Hg) (15,16).
Clinically, the key to diagnosis is a high index of suspicion. Multiple clinical factors, as noted above, will establish the diagnosis. The first clue to abdominal compartment syndrome is a distended and tense abdomen. These patients will frequently demonstrate hemodynamic instability with difficulty ventilating and poor urine output. Examination of the patient's ventilatory status will reveal elevated peak inspiratory pressures, often well above 30 mm Hg. If the patient is ventilated with a pressure-control ventilatory method, he or she will alternatively demonstrate low tidal volumes. As clinical suspicion increases, a bladder pressure may be transduced for definitive diagnosis. An arterial pressure line is attached to the patient's Foley catheter, and approximately 60 mL of sterile saline is introduced. Abdominal pressures greater than 15 mm Hg are indicative of abdominal compartment syndrome. When the transduced pressure reaches 25 to 30 mm Hg, a decompressive laparotomy is indicated as therapy for abdominal compartment syndrome (16,17). Of importance, decompressive laparotomy may be indicated at lower intra-abdominal pressures depending on the patient's clinical condition (18). After decompressing the abdominal contents, the abdomen is left open with a temporary abdominal closure until swelling diminishes enough to allow closure. Although decompressive laparotomy for abdominal compartment syndrome is life-saving, it continues to be associated with a 42% to 68% mortality rate (15) although a lower mortality rate has been reported and is dependent on the severity score (19).
The Open Abdomen
Over the last two decades, management strategies for abdominal domain have changed drastically. Even as few as 15 to 20 years ago, the surgical bias was that the abdomen must be closed at all costs. Two increasingly recognized trends in surgery have led to a change in perspective, where the open abdomen is no longer a catastrophe but rather a tool in the surgeon's armamentarium. First, the increasing recognition of primary and secondary abdominal compartment syndrome has led many surgeons to choose the open abdomen as a management strategy for the short term. Second, “damage control laparotomies” have become increasingly common in treating major abdominal trauma. Although the idea of abbreviated laparotomy was first described by Stone et al. in 1983 (20), the formal nomenclature and increasing popularity are credited to Rotondo et al. in 1993 (21). Damage control laparotomy is aimed at limiting intraoperative times for deteriorating patients, allowing transfer to the intensive care unit for vigorous resuscitation. Intraoperatively, major vascular hemorrhage is controlled, either by ligation or packing, and gross bowel contamination is controlled through ligation, often leaving the gastrointestinal tract in discontinuity. The patient's abdomen is then closed in a rapid and temporary manner, with a plan to return when the patient is more stable to effect definitive repair. Damage control laparotomy remains an aggressive strategy for treatment of patients who develop the deadly triad of coagulopathy, hypothermia, and metabolic acidosis (Fig. 77.2). By definition, it requires use of the open abdomen technique, at least until definitive surgical repair is possible.
The open abdomen, while an appropriate management technique, may ultimately become a Gordian knot. The questions of how to manage an open abdomen, and how and when to close it, may be difficult. Continuing management of the open abdomen involves three primary decision-making stages—initial operative management, decision to close primarily versus a planned ventral hernia, and definitive closure of the planned ventral hernia. At the time of the initial damage control laparotomy, the surgeon must choose to temporarily close the abdomen. The original temporary abdominal dressing is known as the Bogota bag. Initially described from its use in Colombia during the 1980s, it consists of covering the abdominal contents with a sterile saline bag to protect the bowel until re-exploration. A derivation of the Bogota bag is a widely used method of temporary abdominal closure in current practice. A plastic drape, such as a sterile cassette cover, is placed over the bowels to prevent them from injury and to allow drainage of fluid. A sponge or blue towel, with two large Jackson-Pratt drains (Cardinal Health, McGaw Park, IL), is then placed over the plastic drape. The entire system is folded under the fascia to contain the abdominal contents. An adhesive drape is placed over the abdomen to maintain sterility, contain contents, and prevent free drainage of fluid (Fig. 77.3). The drains are placed to suction to allow egress of blood and edema fluid. This dressing is then left intact until return to the operating room (22). This method is preferred to a traditional Bogotà bag, as it allows control of abdominal edema with no significant additional investment in time or supplies in the operating room. Regardless of method, the primary goal at this stage is rapid closure with protection of intra-abdominal contents. The exact technique is the surgeon's choice (19,23).
|
|
|
Figure 77.2. The “bloody vicious cycle” of coagulopathy, hypothermia, and metabolic acidosis. |
|
|
|
Figure 77.3. A temporary abdominal closure, using a sterile cassette cover and drains, as used in our practice. |
After an appropriate resuscitation period, typically 24 to 48 hours, the patient is returned to the operating room. If definitive therapy is complete, the decision to close primarily depends on the quantity of intra-abdominal edema and the quality of the fascia. Whenever possible, primary closure of fascia is ideal. The goal of every closure is to minimize tension on the fascia. High-tension closures not only result in elevated intra-abdominal pressures, but also lead to ischemia of the involved fascia with subsequent breakdown and the risk of dehiscence. If it is not possible to close the fascia, or if further trips to the operating room are indicated, the surgeon should choose a temporary closure that prevents lateral retraction of the fascia and facilitates later primary closure. Vicryl mesh sewn directly to the fascia is a form of temporary abdominal closure that may be pleated later in the intensive care unit. Mesh pleating and wound care may continue until intra-abdominal swelling diminishes and the fascia is near enough to close (15). Alternatively, vacuum-assisted fascial closure may be pursued. The most commonly used system is made by KCI (KCI Wound VAC System, Kinetic Concepts, Inc., San Antonio, TX) and involves a pie-crusted plastic drape with incorporated sponge, a separate wound sponge, and adhesive dressing with suction tubing. In this method, the bowels are protected with the plastic drape containing the incorporated sponge. A specially designed drainage sponge with constant suction is then placed, and the abdomen is covered with an adhesive dressing. The sponge suction provides constant medial tension, without disrupting the fascia, to prevent lateral retraction (22,23). Regardless of which method is chosen, most studies have indicated a high rate of primary closure if the patient has a net negative fluid balance at the time of operation. Therefore, management of the patient's volume status may be as important as the method of temporary closure in allowing later reapproximation of the fascia. However, net negative volume balance is extremely difficult to achieve in critically ill trauma patients requiring large-volume resuscitations. Therefore, a large percentage of these patients will go on to planned giant ventral hernias. In a study by Jernigan et al. (24) in 2003, 42% of patients with temporary closures for hemorrhagic shock ultimately were managed with planned, giant ventral hernias.
Closure of the Giant Ventral Hernia
For those who are not closed primarily, the ultimate management may be with the creation of a giant ventral hernia. These patients are managed for the first 1 to 2 weeks postinjury with Vicryl mesh and dressing changes or vacuum-assisted abdominal closures. Once the abdominal contents display a healthy bed of granulation tissue, the abdomen is given a split-thickness or full-thickness skin graft. The patient is then observed for 6 to 12 months as she or he undergoes rehabilitation and nutritional repletion.
As the ventral hernias are somewhat debilitating and cosmetically displeasing, most patients will be eager for definitive closure of the hernia (Fig. 77.4). The surgeon must consider the patient's nutritional status, as well as the laxity of the skin graft, prior to offering closure. Over time, the skin graft and intra-abdominal adhesions will soften, allowing easier graft removal and adhesiolysis. Rushing to repair a giant ventral hernia will result in operating in a hostile abdomen, with the risk of enterotomies and injury to the patient. As noted above, the ideal window for most patients appears to be at 6 to 12 months (Table 77.1) (25). The repair of the giant ventral hernia is also a good time for repair of any fistulas and reversal of stomas.
|
Table 77.1 Management Options for the Open Abdomen |
||||||||||||
|
||||||||||||
|
|
||||||||||||
|
Figure 77.4. A planned ventral hernia, quite large, ready for definitive repair. |
Most giant ventral hernias will not be amenable to primary closure. Therefore, the surgeon must decide the best method of restoring abdominal domain. The use of mesh is one option but may not be possible if enterotomies are made during the lysis stage or if stoma reversal is necessary. An increasingly popular option for these patients is a full or modified components separation. After sharply removing the skin graft, adhesed small bowel is freed from the overlying fascia for a distance of 4 to 6 cm. Skin flaps are raised laterally on both sides to the level of the midaxillary line to allow placement of relaxing incisions and full mobility of the fascia. When the skin flaps are fully raised, a relaxing incision is made in the external oblique fascia just lateral to the semilunar line. The incision is taken from above the ribs, often requiring division of some muscle, to the level of the pubis. Some additional medial mobility may be gained by dividing the filmy tissue between the external oblique muscle and the overlying fascia. This limited release may be adequate to allow reapproximation of the fascia at the midline. Aggressive closure under tension may lead to respiratory compromise and all the complications associated with abdominal compartment syndrome.
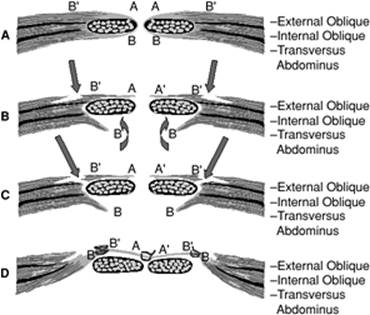
If the fascia will still not come together in a tensionfree manner, a full separation of components is indicated. An incision is made in the anterolateral rectus sheath and the posteromedial rectus sheath bilaterally. The medial posterior sheath is then sewn to the lateral edge of the anterior sheath to provide added length of abdominal wall (Fig. 77.5). When the fascia is closely approximated, it is closed with interrupted PDS (polydioxanone sutures). Four Jackson-Pratt drains are then placed, one superior and one inferior bilaterally, and the skin is closed. Postoperatively, nasogastric suction is maintained until output decreases and drains are left in until output drops to less than 20 mL per day.
|
|
|
Figure 77.5. Depiction of a separation of components repair of a giant ventral hernia. |
|
|
|
Figure 77.6. Definitive closure of a giant ventral hernia. |
Occasionally, despite full separation, the fascia is still not close enough for a tensionfree repair. In these patients, a mesh or AlloDerm interposition may be necessary to achieve closure. This is most commonly seen in the upper portion of the closure where the rib cage may provide some increased lateral tension. Overall, patients tolerate closure well and long-term success is excellent with only a 5% recurrent hernia rate in experienced hands (Fig. 77.6) (24,25).
Short Bowel Syndrome
Short bowel is defined as a gastrointestinal length of 2 m, or less, and the cause may vary greatly between children and adults. Short bowel is an outcome of intra-abdominal catastrophe resulting in extensive surgical resection. Children most commonly end with short gut syndrome following a congenital or neonatal process such as necrotizing enterocolitis, intestinal atresia, volvulus, or gastroschisis. Adults acquire short gut syndrome following extensive surgical resection necessitated by malignancy, trauma, obstruction, or vascular insufficiency. Regardless of the cause, a patient's ultimate outcome is largely determined by the length of remaining small bowel and the presence or absence of the colon. Presence of the colon can extend the functional capacity of the remaining bowel. To have the potential for enteral autonomy, a patient requires at least 150 cm of small bowel, or 60 to 90 cm if the colon is present (26). Presence of the ileocecal valve is also important in maintaining hydration and modulating gastrointestinal transit time.
Short gut syndrome is most obviously defined by difficulty meeting nutritional requirements and dependence on parenteral nutrition. Patients will complain of weight loss, diarrhea, and steatorrhea. On a physiologic level, patients develop gastric emptying abnormalities and rapid transit times due to short intestinal length. Dehydration is a constant threat if the colon is absent due to an inability to reabsorb the approximately 4 L of gastrointestinal secretions per day. Loss of absorption results in deficiencies in B12, fat-soluble vitamins, and bile salts. Short gut patients are also prone to cholelithiasis and nephrolithiasis due to altered absorption of bile salts and oxalate, peptic ulcers due to increased gastric secretions, line sepsis from deep catheters for delivery of parenteral nutrition, and liver dysfunction from that same parenteral nutrition (27).
A surgeon's role in managing short gut starts in the operating room with the very first incision. At the initial operation, the surgeon should make every effort to preserve bowel length, as well as the ileocecal valve. In some cases, it may be safest to limit resection and return at a later date to inspect marginally viable bowel. Initial postoperative therapy is often supportive, as this patient population is critically ill after emerging from the operating room. Early central venous access with immediate institution of parenteral nutrition aids in healing and prevents malnutrition. The long-term management of short gut patients then requires a multidisciplinary team involving physicians and nurses, nutritionists, patients, and their families.
Patients with short gut generally fall into two groups—those with insufficient length (usually less than 45–60 cm) who require lifelong parenteral nutrition and those with adequate length to potentially adapt and become partially or totally enterally independent. Adaptation is a process whereby the absorptive surface of the gut alters to increase digestive capacity and improve nutritional potential. In most cases, the ability is dependent on time and the nature of the remaining bowel. The ileum is capable of adapting to many jejunal functions, but the reverse is less successful (27). Some studies advocate the use of recombinant growth hormone to improve adaptation. In patients who are nutritionally maximized, growth hormone promotes mucosal hyperplasia and increases villous surface area. The process is further enhanced by high-carbohydrate, low-fat diets. Although minimal evidence exists in humans, animal studies have shown enhanced adaptation and nutritional repletion with selective use of growth hormone. Glutamine has also been proven beneficial and works synergistically with growth hormone. Glutamine, and trophic feeds, stimulate enterocytes and enhance cell proliferation. Even in patients who are completely parenterally dependent, low-rate trophic feeds maintain mucosal health (28). Additionally, preservation of colonic length improves fluid reabsorption. This improves patient hydration, leading to a more normal bowel regimen and improving the success of adaptation and weaning from parenteral nutrition. With these facts in mind, surgeons have a number of adjuncts to improve intestinal performance once bowel length is defined.
Occasionally, surgical therapy is required to deal with the sequelae of short gut or to promote adaptation. In patients with enteral continuity who are increasing oral intake, rapid transit due to inadequate length for absorption may result in persistent and disabling diarrhea and worsening of malnutrition. In these cases, conservative therapies such as medication and diet modification are the first line of therapy. If these are inadequate, segmental interposition may be attempted. Ideally, approximately 10 cm of small bowel is reversed and interposed in the gastrointestinal tract. When intraluminal contents reach the reversed segment, the antiperistaltic flow slows transit time. In cases where small bowel length is inadequate, a colonic limb may be interposed. This option is much less favored and rarely performed. Creation of an artificial valve is also a possibility for those lacking a native ileocecal valve. The key to creation of a successful valve is an appropriate length, as one that is too short will have minimal impact on transit time and one that is too long may cause obstruction. An ideal length is felt to be 2 cm although evidence regarding effectiveness is limited, as this is not a commonly performed procedure (29). Of note, surgical therapy for short bowel syndrome is pursued infrequently and is generally referred to tertiary centers with extensive experience managing these challenging patients.
In some cases, patients may have adequate remaining length for enteral independence but suffer from poor function secondary to obstruction, pseudo-obstruction, or dilation. Initial focus should be on relief of the obstruction. Obviously, adhesive bands obstructing the bowel lumen should be dealt with by simple lysis. In some cases, however, the small bowel may demonstrate one or multiple strictures. As bowel length in short gut patients is obviously at a premium, resection with anastomosis is not a good option. To preserve length and relieve obstruction, a stricturoplasty remains a reasonable alternative. In standard Heineke-Mikulicz stricturoplasty, a longitudinal incision is made along the length of the stricture. The enterotomy is then closed in one or two layers in a transverse direction. More involved stricturoplasties may be indicated depending on the specific details of the situation. However, a standard stricturoplasty should be adequate for most circumstances. Alternatively, a dilated, poorly functioning segment of bowel may exist in short gut patients due to distal obstructions, like strictures. When the distal obstruction has been dealt with, the dilated segment(s) may be treated by tapering enteroplasty. In this situation, interrupted Lembert stitches are placed on intact bowel to imbricate the wall and to decrease the caliber of the lumen. All of these procedures have specific indications and are pursued to maximize function of minimal bowel length.
When bowel length is too short, additional centimeters may be gained via a lengthening procedure. This may mean the difference between total parental nutrition dependence and partial enteral autonomy. In lengthening procedures, the antimesenteric border is incised, as well as the mesenteric border. Care must be taken to preserve the blood supply to both sides. Each side is then closed to form parallel tubes. These tubes are anastomosed end to end to create a segment that is twice as long but with a narrower lumen (2). A final option in pursuit of enteral independence is small bowel transplantation. Depending on the patient's hepatic function, a complete small bowel and liver transplant may be required. Small bowel transplantation remains an area of growth and continued challenge in the transplant community. Indications for small bowel transplantation include permanent intestinal failure as demonstrated by occlusion of two or more major veins, frequent episodes of line sepsis, unacceptable quality of life, or liver failure. With current induction and maintenance therapies, the 1-year survival for small bowel transplantation is approximately 65% and is only slightly lower at 59% when liver transplantation is included (30). With early evaluation and referral, specialized centers are achieving much better 2-year survival after small bowel transplantation with less morbidity related to immunosuppressive dosing. Transplant centers have been able to maintain good graft function while weaning patients off steroids and minimizing dosing of the most toxic immunosuppressive agents. Transplant remains an imperfect choice for short gut patients but has increasing promise for patients who have exhausted alternatives.
Radiation Enteritis
Radiation damage to the gastrointestinal organs can be a particularly vexing problem for the surgeon and the patient. Ionizing radiation is delivered neoadjuvantly or adjuvantly for neoplastic processes occurring in organs of the pelvis. Radiation damages mitotically active cells of the mucosal surface epithelium, especially crypt cells. The incidence of injury is dependent on such factors as volume of irradiated small bowel, total dose delivered as well as dose per fraction, and type of radiation being delivered (31). In addition, radiation causes production of oxygen free radicals which further damages tissues at the cellular level. These cellular disruptions manifest as obliterative arteritis with subsequent bowel ischemia. Affected bowels may develop strictures, perforate, or develop fistulas (Fig. 77.7). Additionally, inflammation resulting from injury causes formation of dense local adhesions. Of patients undergoing abdominal and pelvic radiation, 50% to 75% will have some symptoms related to the therapy in the months to years following treatment. The most common symptoms are vague abdominal pain, diarrhea, rectal bleeding, and tenesmus. In 1% to 15%, bothersome symptoms will progress into actual radiation enteritis. Although symptoms most commonly occur during therapy, and may be abrogated by decreasing the radiation dose by 10%, patients may develop chronic radiation enteritis years after treatment. In the case of late radiation enteritis, workup should include dismissing recurrence of the initial neoplasm (2,32).
Initial management of radiation enteritis should embrace conservative measures. Sitz baths and stool softeners are effective initial treatments for rectal and anal symptoms. Opiates, antispasmodics, and anticholinergics will decrease transit time if diarrhea is the primary problem. Steroid enemas and sucralfate (by mouth or by rectum) can diminish irritation of the mucosa, which results in rectal pain and bleeding. If the patient is malnourished from chronic enteritis, total parenteral nutrition (TPN) may be necessary, especially if operative intervention is entertained.
|
|
|
Figure 77.7. The effects of ionizing radiation on gastrointestinal cells and overall small bowel. |
Surgical Therapy for Radiation Enteritis
Surgical therapy for radiation enteritis encompasses two phases—prevention and therapy. If radiation is planned as an adjuvant therapy following surgery, some techniques may be used to diminish radiation injury. Simple nonsurgical methods to diminish radiation injury include patient positioning, multiple field techniques, and bladder distention (31). Following pelvic surgery, reperitonealizing the operative field will diminish local adhesions, which may serve to draw small bowel into the radiation field. Intra-operative efforts are designed to decrease the volume of small bowel included in the radiation field postoperatively. Use of mesh to construct a sling for exclusion of small bowel from the pelvis has had some success. However, this increases the risk of mesh-related hernias with the attendant risk of obstruction or strangulation, the rate of deep venous thrombosis, and the incidence of pelvic fluid collections. Using omentum to exclude the pelvis is rarely an option. This alternative is not available for most patients but has a lower incidence of the aforementioned mesh-related complications. Small bowel displacement systems, though not commonly used, have had some success in physically excluding up to 50% of small bowel volume from the radiation field (31).
The second role of surgery is in the treatment of complications of radiation enteritis. The most common indication for surgery remains obstruction, but other indications include excessive bleeding, intractable diarrhea, pain, fistulas, and persistent abscess. Any surgical intervention should use the least invasive procedure required to address the issue. Excessive handling of radiated tissues commonly results in unplanned enterotomies and may interrupt an already tenuous blood supply. Any suspicious-appearing areas should be biopsied to evaluate for recurrent neoplasm. The diseased segment, if involved in obstruction or fistula, should be excised, and the anastomosis should attempt to include nonradiated bowel. Minimal lysis of adhesions should be pursued to prevent disruption of tenuous blood supplies. If dense adhesions prevent access to the involved segment, a gastrointestinal bypass may be necessary. This option will predispose a patient to blind loop syndrome and bleeding but may be a better option than attempting to mobilize frozen bowel (32).
Approximately 2% to 5% of patients with a history of pelvic radiation therapy will develop chronic proctopathy, which may include rectal pain and bleeding (33). First-line therapies of sucralfate and steroid enemas are of limited benefit. Endoscopic coagulation of bleeding with electrocautery or laser has been successful for limited bleeding sites. Laser photocoagulation has a low morbidity rate of 5% to 15% but requires multiple treatment sessions. The most effective nonoperative therapy remains the topical application of 4% formalin, with 85% of patients responding after two instillations or less (33). When these measures fail, invasive therapy is pursued. If there is a component of stricture, initial therapy should include serial dilation. However, if this is unsuccessful or the indication is intractable pain, severe incontinence, or profound bleeding, a diverting colostomy may be necessary. In worst case situations, abdominoperineal resection may be pursued. In the event of fistulas, the fistula tract and involved tissue at either end must be resected and the sites closed. An interposition flap of omentum or muscle should then be placed to protect the repair sites. Again, prevention is truly the best option for the problem of radiation enteritis. New radiation regimens with lower doses and more specific direction potentially provide the most benefit for this patient population.
Summary
Even the most routine abdominal surgery has the potential for a difficult postoperative course. When postoperative patients do not progress as anticipated, or when complications develop, a high index of suspicion is important for rapid diagnosis and treatment. The cornerstone of every difficult postoperative problem is meticulous and careful technique at the time of the original surgery. Once the problem is manifest, attention to the patient's condition and conservative management are widely favored initial approaches. Ultimate therapeutic choices may have a profound effect on the patient's eventual recovery and quality of life. Whether the final cure is by careful manipulation of patient physiology or by surgical intervention, the critical care surgeon must be well versed in a multitude of complex postoperative issues to provide exceptional and appropriate therapy.
Pearls
· Routes to provide enteral feedings should be considered at the time of surgery for patients in whom oral intake is not anticipated for some time. Either surgical jejunostomy or manual placement of small nasoenteric feeding tubes past the pylorus will help the patients with early nutrition and possible avoidance of parenteral nutrition.
· All tubes and drains must be secured to minimize inadvertent dislodgement. Loss of carefully placed tubes and drains can lead to significant morbidity.
· Avoid re-entering the abdomen in the first 2 to 3 weeks after previous surgery (if possible). This is the peak time for dense adhesions and iatrogenic injury may occur.
· Carefully assess the patient's general condition before entering a hostile abdomen. Cardiovascular and pulmonary status, nutritional support, blood sugar control, and coagulation profile should be optimized if possible.
References
1. Fazio VW, Cohen Z, Fleshman JW, et al. Reduction in adhesive small-bowel obstruction by Seprafilm Adhesion Barrier after resection. Dis Colon Rectum. 2006;49(1):1–11.
2. Cameron JL, ed. Current Surgical Therapy. 7th ed. St. Louis, MO: Mosby; 2001.
3. ten Raa S, van den Tol MP, Sluiter M, et al. The role of neutrophils and oxygen free radicals in post-operative adhesions. J Surg Res. 2006;136(1):45–52.
4. Johns A. Evidence based prevention of post-operative adhesions. Hum Reprod Update. 2001;7(6):577–579.
5. Van't Rient M, de Vos van Steenwijk PJ, Bonthuis F, et al. Prevention of adhesions to prosthetic mesh: comparison of different barriers using incisional hernia model. Ann Surg. 2003;237(1):123–128.
6. Memon AS, Siddiqui FG. Causes and management of postoperative enterocutaneous fistulas. J Coll Physicians Surg Pak. 2004;14(1):25–28.
7. Li J, Ren J, Zhu W, et al. Management of enterocutaneous fistulas: 30-year clinical experience. Chinese Med J. 2003;116(2):171–175.
8. Gray M, Jacobson T. Are somatostatin analogues (octreotide and lanreotide) effective in promoting healing of enterocutaneous fistulas? J Wound Ostomy Continence Nurs. 2002;29(5):228–233.
9. Maconi G, Parente F, Porro GB. Hydrogen peroxide enhanced ultrasound-fistulography in the assessment of enterocutaneous fistulas complicating Crohn's disease. Gut. 1999;45(6):874–878.
10. Draus JM Jr, Huss SA, Harty NJ, et al. Enterocutaneous fistula: are treatments improving? Surgery. 2006;140(4):570–578.
11. Pannegeon V, Pessaux P, Sauvanet A, et al. Pancreatic fistula after distal pancreatectomy: predictive risk factors and value of conservative treatment. Arch Surg. 2006;141(11):1071–1076.
12. Kaman L, Behera A, Singh R, et al. Internal pancreatic fistulas with pancreatic ascites and pancreatic pleural effusions: recognition and management. ANZ J Surg. 2001;71(4):221–225.
13. Kron IL, Harman PK, Nolan S. The measurement of intra-abdominal pressure as a criterion for abdominal reexploration. Ann Surg. 1984;199(1):28–30.
14. Reed SF, Britt RC, Collins J, et al. Aggressive surveillance and early catheter-directed therapy in the management of intra-abdominal hypertension. J Trauma. 2006;61(6):1359–1365.
15. Maxwell RA, Fabian TC, Croce MA, et al. Secondary abdominal compartment syndrome: an underappreciated manifestation of severe hemorrhagic shock. J Trauma. 1999;47(6):995.
16. Crandall M, West MA. Evaluation of the abdomen in the critically ill patient: opening the black box. Curr Opin Crit Care. 2006;12(4):333–339.
17. Ivatury RR. Abdominal compartment syndrome: a century later, isn't it time to accept and promulgate? Crit Care Med. 2006;34(9):2494–2495.
18. DeWaele JJH, Malbrain EA, Lng M. Decompressive laparotomy for abdominal compartment syndrome—a critical analysis. Crit Care. 2006;10(2):R51.
19. Malbrain MLNG, Chiumello D, Pelosi P, et al. Incidence and prognosis of intraabdominal hypertension in a mixed population of critically ill patients: a multiple-center epidemiological study. Crit Care Med. 2005;33:315.
20. Stone HH, Strom PR, Mullins RJ. Management of the major coagulopathy with onset during laparotomy. Ann Surg. 1983;197:532–535.
21. Rotondo M, Schwab CW, McGonigal MD, et al. Damage control: an approach for improved survival in exsanguinating penetrating abdominal injury. J Trauma. 1993;35:375–383.
22. Stone PA, Hass SM, Flaherty SK, et al. Vacuum-assisted fascial closure for patients with abdominal trauma. J Trauma. 2004;57(5):1082–1086.
23. James C, Stawicki SP, Hoff WS, et al. A proposed algorithm for managing the open abdomen. Am Surg. 2005;71(3):202–207.
24. Jernigan TW, Fabian TC, Croce MA, et al. Staged management of giant abdominal wall defects: acute and long-term results. Ann Surg. 2003;238(3):349–357.
25. Fabian TC. Damage control in trauma: laparotomy wound management acute to chronic. Surg Clin North Am. 2007;87:73–93.
26. DiBaise JK, Matarese LE, Messing B, et al. Strategies for parenteral nutrition weaning in adult patients with short bowel syndrome. J Clin Gastroenterol. 2006;40(Suppl 2):S94–98.
27. Nightingale J, Woodward JM. Guidelines for management of patients with a short bowel. Gut. 2006;55(Suppl 4):1–12.
28. Steiger E, DiBaise JK, Messing B, et al. Indications and recommendations for the use of recombinant human growth hormone in adult short bowel syndrome patients dependent on parenteral nutrition. J Clin Gastroenterol. 2006;40(Suppl 2):S99–106.
29. Thompson JS. Surgical aspects of the short-bowel syndrome. Am J Surg. 1995;170(6):532–536.
30. Dijkstra GR, Rings EHHM, van Dullemen HM, et al. Small bowel transplantation as a treatment option for intestinal failure in children and adults. Ned Tijdschr Geneeskd. 2005;149(8):391–398.
31. Park W, Huh SJ, Lee JE, et al. Variation of small bowel sparing with small bowel displacement system according to the physiological status of the bladder during radiotherapy for cervical cancer. Gynecol Oncol. 2005;99(3):645–651.
32. Onodera H, Nagayama S, Mori A, et al. Reappraisal of surgical treatment for radiation enteritis. World J Surg. 2005;29(4):459–463.
33. Cullen SN, Frenz M, Mee A. Treatment of hemorrhagic radiation-induced proctopathy using small volume topical formalin instillation. Aliment Pharmacol Ther. 2006;23(11):1575–1579.