Thomas M. Kessler1 , Stefan De Wachter2 and Marcus J. Drake3
(1)
Neuro-Urology, Balgrist University Hospital, Zürich, Switzerland
(2)
Department of Urology, University Hospital Antwerpen, Edegem, Belgium
(3)
School of Clinical Sciences, University of Bristol, Bristol, UK
Thomas M. Kessler (Corresponding author)
Email: tkessler@gmx.ch
Stefan De Wachter
Email: stefan.dewachter@ua.ac.be
Marcus J. Drake
Email: marcus.drake@bui.ac.uk
Introduction
The control of the lower urinary tract is a complex, multilevel process involving both the peripheral and central nervous system. Thus, lower urinary tract dysfunction (LUTD) is very common in neurological patients resulting from the profound alterations of lower urinary tract control caused by the underlying disease. It is of utmost importance not only to appropriately assess LUTD but also to understand the neurological cause, as it significantly influences the choice of treatment.
What Do the Guidelines Say?
According to the Guidelines on Neuro-Urology of the European Association of Urology (EAU), the aims of neuro-urological management include enhancing quality of life, preservation of upper urinary tract function, control of urinary tract infection and maintenance of a low-pressure bladder that is both continent and capable of emptying completely. Ideally these goals are achieved without an indwelling catheter or a stoma and in a manner that is socially and vocationally acceptable to the patient, whilst avoiding complications such as recurrent urinary tract infections, urethral strictures, calculus disease, hydronephrosis and renal failure.
History taking is the cornerstone of neurogenic LUTD assessment. It needs to gather information on congenital and neurological abnormalities, prior urogenital complications and treatments, medication and urinary tract, sexual, bowel, neurological and gynaecological function. Evaluation of lifestyle factors, such as smoking, alcohol or addictive drugs, and quality of life are also important, and attention should be paid to physical and mental handicaps.
Bladder diary is a highly useful tool in clinical practice as it provides an objective measure of lower urinary tract symptoms (LUTS) mirroring day-to-day reality. In contrast, the patients’ symptoms often cannot be reproduced by clinical examination and urodynamics because of the extraordinary situation and the time limits of medical consultation.
Physical examination includes the abdomen, flanks and external genital organs, as well as sensation and reflexes in the urogenital area (Fig. 2.1). Anal sphincter and pelvic floor functions must be tested extensively. Urinalysis and urinary culture, blood chemistry (if not already performed by the referring physician), free uroflowmetry and post-void residual measurement, either by ultrasound or catheterisation, are part of a basic neuro-urological assessment.
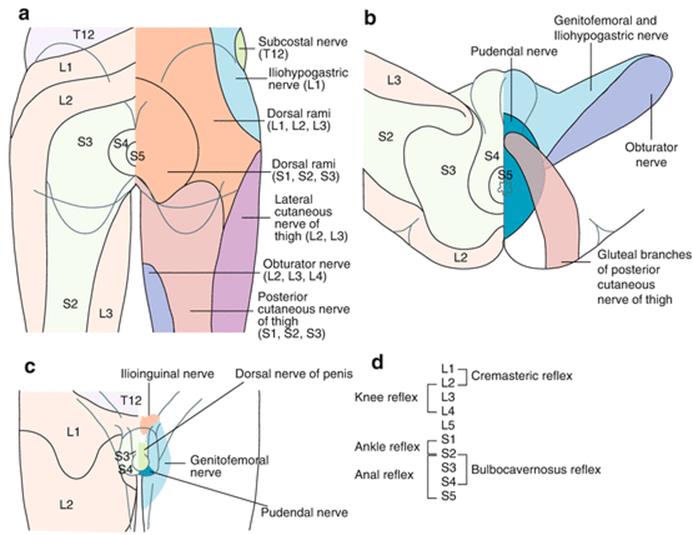
Fig. 2.1
Lumbosacral dematomes, cutaneous nerves, and reflexes. (Panicker JN et al. Lancet Neurol 2015)
Urodynamic investigation, with simultaneous fluoroscopic monitoring (i.e., video-urodynamics), is essential to assess detrusor and bladder outlet function, and it is crucial for clinical decision making. Generally accepted risk factors jeopardising the upper urinary tract are high detrusor pressure during storage phase due to low-compliance bladder and/or detrusor overactivity combined with detrusor sphincter dyssynergia, and urodynamic investigations are needed to identify these conditions.
Urethrocystoscopy (combined with bladder washing cytology if appropriate) is used if indicated to detect urethral and bladder pathologies, such as urethral stricture, urethral or bladder stones and bladder tumours, including carcinoma in situ.
Serum creatinine, cystatin c and corresponding estimations yield a reasonable estimation of renal function with minimal cost and inconvenience. Creatinine clearance provides a more accurate assessment but involves a 24-h urine collection to measure creatinine excretion. This may result in underestimation of renal function if the urine collection is incomplete. The most accurate measurement is isotopic glomerular filtration rate, especially when renal function is poor or with alterations of muscle mass (as is common in patients with neurological disease).
Clinical Practice
A very simple classification system for use in daily clinical practice is provided in (Fig. 2.2
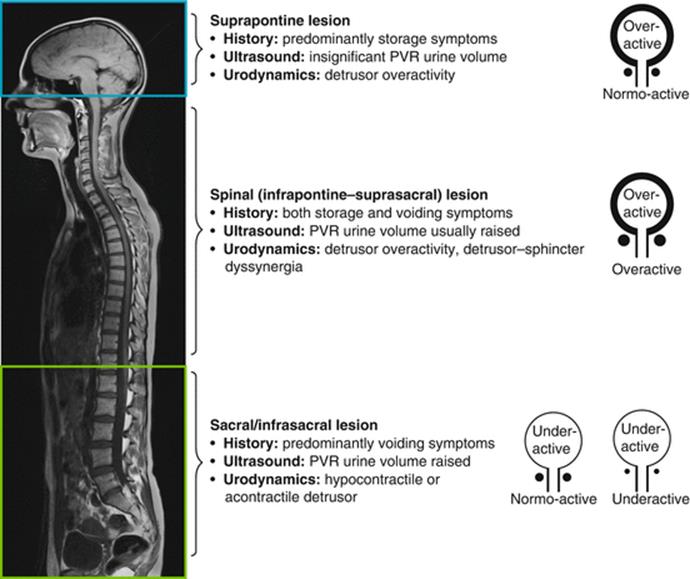
Fig. 2.2
Patterns of lower urinary tract dysfunction following neurological disease. (Panicker JN et al. Lancet Neurol 2015)
). Based on the dysfunction pattern, the appropriate therapeutic strategy to preserve both upper and lower urinary tract function, and to achieve or maintain urinary continence, is determined.
In patients with detrusor overactivity, the therapeutic concept is to convert the overactive detrusor into a normoactive or underactive one. Commonly, antimuscarinics are the pharmacological treatment of choice, but they have limited effectiveness and many patients discontinue their use due to adverse events. The beta-3 adrenergic agonist mirabegron has recently been introduced as an alternative to antimuscarinics for treatment of idiopathic overactive bladder, but research into its application in neurogenic LUTD has not been reported thus far. For refractory neurogenic detrusor overactivity, intradetrusor onabotulinumtoxinA injections are a highly effective, minimally invasive and generally well-tolerated treatment that improves health-related quality of life. In the case of failed onabotulinumtoxinA treatment, augmentation cystoplasty is a well-established treatment option but requires abdominal surgery with interposition of an intestinal segment (usually ileum) into the bladder and/or partial replacement of bladder by an intestinal substitute. In highly selected patients, cystectomy with continent or incontinent urinary diversion becomes necessary as a salvage procedure.
In patients with underactive/acontractile detrusor and/or with detrusor sphincter dyssynergia, intermittent self-catheterisation is recommended to assist bladder emptying. Passive voiding by abdominal straining (Valsalva manoeuvre) or, particularly, by suprapubic downwards compression of the lower abdomen (Credé manoeuvre) is not recommended as it creates high, unphysiological intravesical pressure which puts the upper urinary tract at risk and causes compression of the urethra, i.e. a functional obstruction that leads to inefficient emptying. Nevertheless, some patients are not able and/or not willing to perform intermittent self-catheterisation, and therefore, an indwelling transurethral or suprapubic catheter is potentially the only alternative.
In the case of stress urinary incontinence due to low bladder outlet resistance, electrical stimulation of the pelvic floor can help to restore urinary continence in patients with incomplete lesions. In some neurological patients, the implantation of a sub-urethral sling or an artificial urinary sphincter may become necessary. However, it needs to be considered that artificial urinary sphincters generally do not continue working indefinitely and may need to be replaced with increased risks for revision surgery.
Regular follow-up is essential since neurogenic LUTD is often unstable and symptoms might vary considerably even within a relatively short period. The EAU Guidelines on Neuro-Urology provide clear-cut grade A recommendations that any significant clinical changes should instigate further specialised investigation and that in high-risk patients, the upper urinary tract should be assessed at least every 6 months, physical examination and urinalysis should take place every year, and urodynamics should be done at regular intervals. However, there is a complete lack of high-evidence level studies on which to base such recommendations. Thus, follow-up of the neuro-urological patient is more eminence- than evidence-based. There is no uniform follow-up, and a rather individualised, patient-tailored approach aiming to achieve an optimal quality of life and to protect the upper urinary tract is needed for this special population.
Spina Bifida
Background
Although spina bifida is one of the most common birth defects of the spine, the exact mechanisms resulting in closure or a dysraphic state are yet to be elucidated. Nevertheless, the aetiology of closure defects of the neural tube is supposed to be multifactorial, including both genetic and environmental factors. The deficit of folic acid in the early pregnancy period is a major risk; the role of folic acid in the prevention of neural tube defects has been established since the early 1990s. Maternal ingestion of 400 μg of folic acid per day in all women of child-bearing age can reduce the incidence of spina bifida by 50 %. In the United Kingdom and Ireland, the yearly prevalence of neural tube defects declined, predating any periconceptional folic acid supplementation policy initiatives from 4.5 per 1000 births in 1980 to 1–1.5 per 1000 in the 1990s.
In spina bifida patients, the neurological findings can vary from the most discrete deficit to a complete paraplegia potentially involving all levels of the spinal column. Most spinal defects occur at the lumbar spine with the sacral, thoracic and cervical areas, in decreasing order of frequency, less affected. Associated Arnold-Chiari malformation is seen in more than 80 % of spina bifida children mostly requiring ventriculoperitoneal shunt placement. Whilst the likelihood of bladder, bowel and pelvic floor dysfunction depends on the severity of the lesion, the pattern of the dysfunction is aligned to the localisation.
Neurogenic LUTD in children with spina bifida can lead to secondary upper urinary tract deterioration and often causes chronic urinary incontinence. The preservation of renal function is the primary goal in the neuro-urological management of spina bifida patients, but considering the impact on quality of life, efforts to promote urinary continence have become more and more important. Continence is associated with better self-concept, and incontinent girls are particularly at high risk for poor self-esteem. Urinary incontinence is a stress factor for these patients, and even a slight improvement in urinary continence means to these patients additional independence. Thus, reducing the frequency of incontinence or, even better, the achievement of continence is an important goal of urological medical care.
According to Verhoef et al., urinary and faecal incontinence is common in young adults with spina bifida (61 % and 34 %, respectively) regardless of bladder and bowel management they used. The majority of urinary and faecal incontinent patients perceived this as a problem (70 % and 77 %, respectively). Moreover, the authors of this study found that patients with a level of lesion at L5 or above were far more likely to be urinary and faecal incontinent than those with a level of lesion of S1 or below. However, patients with a level of lesion at L5 and above were also more likely to perceive urinary incontinence as a problem. It is well known that urinary incontinence in these patients has an underlying component of detrusor overactivity and/or poor bladder compliance, which is more frequent in patients with intact or at least partially intact sacral reflexes, which are mostly present in lesions at L5 and above (suprasacral lesion). Remarkably, whilst in utero closure of spina bifida decreased rates of ventriculoperitoneal shunting and improved motor function, it seems not to be associated with a relevant improvement in lower urinary tract function compared to repair after birth.
Points of Interest
Although some authors have questioned the value of urodynamics shortly after birth and serially thereafter, most authors agree that early urodynamics are a prerequisite for an adequate treatment strategy.
The Innsbruck approach, based on more than 30 years of experience with spina bifida patients, is an early proactive conservative management which is the state of the art nowadays. This improves upper urinary tract function and reduces the need for surgery in patients with myelomeningocele in the long term. The initial evaluation consists of a history, neuro-urological examination (especially including bulbocavernosus reflex, anal reflex, anal sphincter tone), urinalysis, urine culture, sonography of kidneys and bladder, as well as (video-) urodynamics. Patients undergo initial evaluation as early as possible, ideally at the day of birth or within 2 weeks after closure of the spina bifida defect. Voiding cystourethrography and urodynamics are performed concurrently as video-urodynamics. Patients at risk for upper urinary tract damage (low bladder compliance, intravesical pressure >40 cmH2O, detrusor sphincter dyssynergia) and those with abnormal findings on imaging studies (trabeculated bladder ± pseudodiverticula, vesico-uretero-renal reflux, dilated ureter, hydronephrosis, cortical thinning/scarring of renal parenchyma) undergo nuclear renal scan. Periodic reassessment with neuro-urological examination, urinalysis, urine culture, imaging studies and (video-) urodynamics are performed every 3–6 months up to age 2 and in yearly intervals thereafter.
Therapeutic strategies for treating neurogenic LUTD in spina bifida patients are in line with those of other neurological disorders mentioned above (see section “Clinical practice”). It should be considered, however, that latex allergy is very common in this population, and latex avoidance in children is strongly recommended as it seems also to prevent sensitisation to other allergens and allergic diseases which might be explained by the prevention of sensitisation spreading. In addition, due to the congenital nature of the disease, the patients cope since birth with the disability and spina bifida children have a lower self-concept than their peers with typical development, what may also become relevant for adolescence and adulthood.
Spinal Cord Injury
Background
Spinal cord injury (SCI) is a devastating event with far-reaching consequences for the individual’s health and the family’s economic and social future. It affects each year 15–40 new individuals per million in Western countries and will result in neurogenic LUTD in most of these patients. In the past, renal disease was responsible for more than 40 % of deaths following SCI. The introduction of intermittent self-catheterisation and the use of regular urodynamic investigations have since revolutionised the neuro-urological care of SCI patients. Hence, nowadays, urinary disease accounts for only about 13 % of deaths in SCI patients, and the most common cause of death now is related to pneumonia. It follows that adequate function of the urinary tract is essential to prevent morbidity and mortality in SCI patients.
Despite the fact that improved management of neurogenic LUTD has dramatically decreased morbidity and mortality in SCI patients, many important issues still remain. The patho-mechanisms involved in neurogenic LUTD are incompletely understood and many hypotheses established in animal models have not been proven in humans. Acute SCI lead to a state named “spinal shock”: Muscles are generally in a flaccid state because of the loss of neurological reflexes, and urinary tract function is characterised by detrusor acontractility and urinary retention/voiding dysfunction. After a period of time of usually around 4–12 weeks, detrusor overactivity mostly combined with detrusor sphincter dyssynergia develops in the case of a suprasacral lesion (today the vast majority of SCI) as a result of reorganisation of neuronal circuitry. Disconnection from supraspinal centres means that voiding is not centrally driven but induced by volume-determined reflex detrusor connections. Detrusor sphincter dyssynergia may lead to high bladder pressures jeopardising the upper urinary tract. The emergence of these dysfunctional patterns is a complex, not yet fully understood process, but C-fibre-mediated spinal reflex pathways seem to be involved.
In contrast to chronic SCI, little is known about LUTD patterns during the acute phase of SCI, probably because urodynamic investigations are postponed to the chronic phase or are not performed at all, especially in patients with less well-pronounced neurological impairments. However, in a recent prospective study investigating neurogenic LUTD due to acute SCI (duration of injury less than 40 days), unfavourable urodynamic parameters, i.e. high-pressure system during storage phase, low-compliance bladder, detrusor overactivity, detrusor sphincter dyssynergia and vesico-uretero-renal reflux, were found in an unexpectedly high percentage of 60 % of the patients. Remarkably, ambulatory and nonambulatory patients had a similar risk of unfavourable measures so that same neuro-urological assessment including urodynamic investigations are strongly recommended in all acute SCI patients independent of the ability to walk.
In addition, SCI is not a stable condition, and so neuro-urological treatment strategies need to be flexible as they often need to be modified in almost all patients throughout life.
Points of Interest
Ideally, SCI patients should be managed in specialised SCI centres. The involvement of the neuro-urologist should not be confined to managing LUTD but should extend to addressing sexual dysfunction, fertility if relevant and bowel dysfunction.
In patients with complete SCI, sacral anterior root stimulation can be used to permit voiding but also requires sacral posterior root rhizotomy (also known as dorsal rhizotomy or sacral deafferentation) to suppress detrusor overactivity. Nowadays, sacral anterior root stimulation is rarely used as patients are reluctant to undergo concomitant dorsal rhizotomy which is a destructive, irreversible procedure resulting in the loss of reflex sexual function and reflex defecation. This is not ideal especially considering that the other minimally invasive options are available.
Of great interest is a recent study on the use of early bilateral sacral neuromodulation in patients with complete SCI during the spinal shock. Data suggest that this treatment could prevent the development of detrusor overactivity and urinary incontinence as well as improve sexual and bowel function. If the benefits of early sacral neuromodulation can be proven in randomised trials and if these findings are conveyed to other neurological disorders, then the management of neurogenic LUTD will be revolutionised. Adequately designed clinical studies will be required to confirm what looks to be a promising future in the field of neuro-urological care following SCI.
Autonomic dysreflexia is a sudden and exaggerated autonomic response to stimuli in patients with SCI or spinal dysfunction generally above level T6. Hypertension is a relatively common manifestation of autonomic dysreflexia and can have life-threatening results if not properly managed.
Multiple Sclerosis
Background
Multiple sclerosis (MS) is an acquired inflammatory disease in which the myelin sheath of nerve cells in the brain and spinal cord are damaged, leading to a diverse range of signs and symptoms. Symptoms can either occur in isolated attacks (relapsing MS) or steadily accumulate over time (progressive MS). Between attacks, symptoms may largely recover, but cumulative damage does steadily reduce patients’ overall functional abilities. The cause of MS is unknown, but autoimmune mechanisms may be relevant. Genetic predisposition and environmental factors, e.g. infection, have been proposed. The disease usually begins between the ages of 20 and 50 and is twice as common in women as men. There is no current curative treatment, and disease modification to reduce progression is the current strategy. Life expectancy is reduced in comparison to an unaffected population.
Neurogenic LUTD has a profound effect on quality of life in patients with MS. Typically, it becomes apparent at a comparatively early stage in the progression of the illness, and it can be a presenting feature of MS. Ultimately, LUTD affects a high proportion of MS patients, the occurrence being influenced by the type of MS, the duration of the illness, and the degree of disability. Storage LUTS are the most common urinary symptoms in MS, including increased daytime frequency, urgency, nocturia and urgency incontinence. Nonetheless, voiding dysfunction can be present at an early stage, and post-void residuals are common, whilst acute urinary retention can occur. Unfortunately, LUTD is often overlooked in MS, since urological input is not widely available in the care pathway for these patients. Consequently, diagnosis of preventable or correctable urological complications may be somewhat delayed. This is particularly the case in more advanced MS. The exact type of LUTD typically reflects the extent of the central nervous system affected by MS, and thus predictably can alter with any episode of disease relapse or progression, necessitating re-evaluation.
Alongside symptom management, potential complications affecting the upper urinary tract include renal calculi, hydronephrosis or vesico-uretero-renal reflux. Severe renal insufficiency is comparatively unusual in patients with MS. Nonetheless, some degree of renal insufficiency is a feature of more advanced cases of MS. An analysis of causes of death on death certificates in the United States of America showed a comparatively low prevalence of severe renal dysfunction. In fact, symptomatic urinary tract infection was listed as a contributing factor in 8.4 % of deaths, and this is one of the key management aspects for urological care in MS, with about two thirds of patients reporting at least one urinary tract infection annually. This may reflect the known high prevalence of asymptomatic bacteriuria in many neurological patients.
As a general principle in neuro-urology, video-urodynamics primarily aims to identify risk factors that may affect patient safety, with symptom management being very important but secondary. Urodynamic findings in MS can take many forms. Detrusor overactivity or stress urinary incontinence is well recognised during the storage phase, whilst detrusor underactivity or detrusor sphincter dyssynergia can affect voiding. The issues considered most concerning for subsequent problems of the upper urinary tract are impaired filling compliance, detrusor overactivity (especially in the presence of vesico-uretero-renal reflux) and clear-cut detrusor sphincter dyssynergia. Problematically, whilst video-urodynamics is a crucial part of evaluation, the exact risk associated with specific dysfunctions is not well defined. Rather disparate approaches are commonplace in MS assessment, either using video-urodynamics systematically and routinely as a surveillance test or pragmatically and reactively in the event of apparent risk of deterioration.
Points of Interest
Baseline function needs to be documented, and routine follow-up is required, with responsive support available in the event of persisting change in disease status. Patients should have urine checked regularly using dipstick urinalysis, and post-void residual should be screened. Frequency of renal function blood tests or upper urinary tract imaging should be individualised, largely based on disease severity and progression.
Urinary storage symptoms require management with fluid advice, behavioural adaptation, home adaptation and pharmacotherapy. Antimuscarinics are routinely used in MS. Nocturia can be managed with desmopressin if baseline serum sodium level is normal, and early checks of sodium levels are put in place on initiation of treatment. In many patients, storage function is improved by introducing intermittent self-catheterisation to counteract post-void residual. Intermittent self-catheterisation is generally well tolerated in MS, since manual dexterity and trunk control (balance) are usually sufficiently preserved, and urethral sensation is often somewhat reduced.
The use of intradetrusor onabotulinumtoxinA injections in neurogenic LUTD is largely based on high-level prospective clinical studies in MS, which formed the main study group alongside SCI patients. This is now the mainstream treatment of neurogenic LUTD in refractory bladder problems for MS patient able to undertake intermittent self-catheterisation or accept an indwelling urinary catheter.
Parkinson’s Disease and Multiple System Atrophy (MSA)
Background
Parkinson’s disease (PD) is a progressive acquired condition leading to movement disorder, caused by degeneration of dopaminergic neurons in the substantia nigra, along with a loss of dopamine-containing nerve terminals in the basal ganglia. Consequently, skeletal muscle control is affected, and additional consequences are seen for autonomic function, particularly affecting the gastrointestinal and urinary tracts. The basal ganglia generally maintain inhibitory influence promoting urine storage, so PD is commonly associated with detrusor overactivity. LUTD is highly prevalent in PD, giving rise to storage LUTS, voiding LUTS or both. The prevalence of LUTS appears to correlate with severity of the disease, but not so much with the duration. For most patients, the LUTD is evident after the motor disorder. LUTD substantially affects the quality of life in patients with PD. Bladder dysfunction generally correlates with the severity and stage of disability. Nocturia is highly prevalent. Voiding LUTS appears to be less prevalent, and post-void residual is generally not substantially elevated. Urodynamically, detrusor overactivity, bladder outlet obstruction or detrusor underactivity may be seen in PD. Failure of sphincter relaxation may reflect bradykinesia in the bladder outlet, rather than true detrusor sphincter dyssynergia.
Multiple system atrophy (MSA) is a rare, adult-onset progressive degenerative disease of the nervous system, with particular features of autonomic failure. The latter leads to impaired vascular control, LUTD and erectile dysfunction. A neurological picture similar to PD may be seen, but response to PD treatment is poor. Alternatively, cerebellar dysfunction may be the more prominent neurological pattern. MSA is the modern term incorporating the three conditions of striatonigral degeneration, sporadic olivo-ponto-cerebellar atrophy and Shy-Drager syndrome. Glial cytoplasmic inclusions are a diagnostic feature. A high proportion of patients with MSA develop urinary symptoms, either prior to or at the time of presentation with the motor disorder. A study of the urological symptoms in MSA patients found difficulty voiding in 79 %, nocturia in 74 %, sensation of urgency in 63 %, urgency incontinence in 63 %, diurnal urinary frequency in 45 %, enuresis in 19 % and urinary retention in 8 %. Post-void residual appears to increase progressively with longer duration of MSA, and urodynamically, the initial dominance of detrusor overactivity progresses towards poor storage compliance and areflexia. Sphincter electromyography can be a useful part of diagnostic testing, which may distinguish MSA from PD.
Points of Interest
For known PD or MSA, initial assessment follows the lines of other neurological conditions causing LUTD. Clinicians should also be aware that urinary symptoms can be the presenting complaint in MSA and should consider screening for postural hypotension and erectile dysfunction in case of the possibility of undiagnosed MSA being present.
Antiparkinsonian medication may affect LUTD in PD, but beneficial effects are not reliable. Indeed, treatment adjustments that help motor symptoms may actually have a counterproductive symptomatic effect on LUTD. Centrally acting anticholinergics to treat the PD should not be confused with the peripherally acting antimuscarinics used to treat detrusor overactivity. Most neurologists are accepting of this latter indication, feeling that impact on the PD itself is generally marginal; however, it is essential to consider this aspect and a good practice to liaise with the patient’s neurologist if considering such a prescription. Cognitive adverse events resulting from central nervous system influence of antimuscarinics used for LUTD can be important.
Deep brain stimulation is another treatment for the movement disorders of PD, and this can also influence the LUTD. Intradetrusor botulinum toxin A injections have been evaluated for treating intractable detrusor overactivity in patients with PD. This is likely to increase the chance of needing intermittent self-catheterisation, which is otherwise rather unusual in PD.
Recommendations for surgical intervention in PD are generally conservative, particularly in the context of stress urinary incontinence in women, or voiding LUTS in men, in view of the apparent risk of adverse outcomes. In particular, clear attribution of bladder outlet obstruction to benign prostate enlargement requires video-urodynamics, since very similar high-pressure slow-flow traces can reflect various causes of bladder outlet obstruction including neurogenic LUTD. Likewise, surgery should be employed very cautiously in MSA. For example, incontinence is very common after prostatectomy in these patients. In MSA, a tailored approach using conservative measures to treat storage and voiding dysfunction is the mainstay of treatment.
Cerebrovascular Accident
Background
Cerebrovascular accident (CVA) is a highly prevalent, acquired, nonprogressive neurological impairment caused by vascular occlusion or haemorrhage. The initial deficit may improve as a result of plasticity of the central nervous system, leading to partial recovery of function using alternative neural pathways. At the time of maximal impairment following a CVA, 41 % of patients (46 % of women and 37 % of men) had urinary incontinence in one study. Urinary incontinence in the early stages of CVA recovery may be a prognostic indicator for poor survival and ultimate functional dependence. A high proportion remain incontinent at 6 months after the CVA, with effective treatment being important.
At 3 months, a range of LUTS can be reported, including nocturia, urgency incontinence and voiding dysfunction. Right cerebral hemisphere lesions have been linked to LUTD, but not all studies support a hemispheric predominance. Urinary incontinence in stroke patients may reflect loss of central inhibition, allowing emergence of detrusor overactivity. However, impaired bladder sensation (the conscious perception of subconscious sensory information) may also be a factor; this is more a feature of parietal lobe lesions. With acute brainstem stroke, voiding difficulty (28 %) or urinary retention (21 %) outweigh urinary incontinence (8 %). Urodynamically, detrusor overactivity is prevalent but detrusor sphincter dyssynergia is not expected (since CVA generally affects cortical function and brainstem function is usually, but not invariably, preserved).
Points of Interest
Basic diagnosis comprises history and examination, urinalysis, post-void residual assessment and a bladder diary. Immediately after the CVA, an indwelling urinary catheter may be needed to deal with initial LUTD pending recovery. The catheter should be removed at the earliest reasonable opportunity, but intermittent self-catheterisation may be needed if there is a large post-void residual. If incontinence is present, containment should be provided. Rehabilitation involves behavioural therapy, perhaps with antimuscarinics and pelvic floor muscle re-education. Botulinum toxin A injections may not be beneficial.
Intervertebral Disc and Failed Back Surgery
Background
Intervertebral disc prolapse is a prevalent condition that may give rise to neurological damage due to mechanical compression of the spinal cord or of the nerve fibres exiting the cord. In an early stage, stretching of the nerves may lead to irritation and detrusor overactivity, whereas when the disease progresses and becomes chronic, progressive atrophy of the fibres occurs with trophic changes and nerve demyelination resulting in an acontractile/hypocontractile detrusor. Aside from mechanical compression, disc prolapse may also impair nerve function by interfering with the blood flow leading to congestion and ischemia of the nerve roots.
Disc prolapse can occur at any level, but most frequently it occurs at the lumbar spine, followed by the cervical and thoracic spine. Depending on the level, the length and severity of compression, the clinical findings may differ. In general, prevalence of LUTS in patients with disc prolapses varies between 20 and 68 %. Cervical disc prolapse is most often characterised by detrusor overactivity with or without detrusor sphincter dyssynergia, which may lead to high detrusor pressures during storage phase jeopardising the upper urinary tract. Thoracic disc prolapse is less prevalent and leads to neurogenic LUTD in 25–35 % with storage LUTS being most common. The vast majority of disc prolapses occur at the lumbar or lumbosacral level, predominantly at L4/L5 and L5/S1. The spinal cord terminates at the midlevel of L1 forming the conus medullaris. Disc prolapses at the upper lumbar levels may therefore compress the terminal part of the spinal cord, whereas lower lumbar level disc prolapses may cause damage to the cauda equina. Sacral nerves are affected in 1–15 % of the patients with lumbar disc protrusion, and in around 25 %, an acontractile detrusor is found leading to impaired bladder emptying and urinary retention. However, detrusor overactivity also has been described in up to 25–50 % of patients with conus medullaris or cauda equina lesions and has been linked to early disc protrusion and irritation of the nerve roots. Depending on the underlying changes, patients may present with complaints suggestive of obstructive voiding and stress incontinence due to overflow or lack of resistance at the level of the external urethral sphincter, or they may present with complaints of urgency incontinence. Urodynamics reveal a prevalence of neurogenic LUTD between 25 and 75 % in these patients.
Points of Interest
Intervertebral disc prolapse usually includes somatic complaints such as paresthesia of the limbs, muscle weakness and back pain, which should raise suspicion for possible urological dysfunctions. However, LUTS may be the sole presenting symptom in some patients, making the diagnosis of spinal cord or cauda equina compression more difficult. Clinical neurological examination can be very informative in these patients. Disturbed or loss of touch sensation of the perineum or perianal area (saddle anaesthesia) and an altered bulbocavernosus reflex are often found and suggestive of nerve impairment. Furthermore, absence of perianal sensation may be considered a negative prognostic factor for recovery of bladder function after removal of the disc prolapse. If patients are still able to void spontaneously, uroflowmetry quite often shows a reduced maximum and mean flow rate, although a normal flow does not exclude presence of LUTD. Presence of an undulating flow is suggestive for the use of abdominal pressure during voiding.
Urodynamics form the cornerstone in the diagnostic workup, as they allow a detailed evaluation of both storage and voiding phase. Specific attention should be given to the presence or absence of detrusor overactivity and the perception of bladder filling. A reduction in bladder compliance has been reported in up to 30 % of the patients. Furthermore, a reduction of the maximum urethral closure pressure can be indicative of pudendal nerve damage in patients with a conus medullaris or cauda equina lesion.
Cystoscopy is by some considered as informative as urodynamics in patients with disc prolapse and neurogenic LUTD. The combination of decreased sensation of urethral passage of the cystoscope, a changed perception of bladder fullness and absence of cystoscopic signs of obstruction in patients with impaired bladder emptying should raise suspicion for a possible lumbar or lumbosacral disc prolapse and subsequent neurogenic impairment.
Electromyography evaluates the pelvic floor activity and the integrity of the sacral reflexes. Furthermore, the use of concentric needle electromyography provides the possibility for separate analysis of the external urethral and external anal sphincter, which may be useful in cauda equina lesions to evaluate involvement of specific nerve roots.
Treatment of the herniated discs may improve bladder function, although the exact percentage of patients showing normalisation is unknown, due to the difficulty in evaluating the immediate and long-term results, as well as the lack of correlation between improvement of complaints and functional recovery as shown by the different test methods. Improvement of LUTD upon disc surgery has been reported in 20–64 % of the patients, but deterioration of bladder function postoperatively has also been described, ranging from 10 to 60 %. If recovery occurs, it may take years. Therefore, besides treatment of the disc prolapse, specific urological management and close follow-up are warranted. In general, neuro-urological strategies are in line with those of other neurological disorders mentioned above (see section “Clinical practice”).
Further Reading
Fowler CJ, Griffiths D, de Groat WC. The neural control of micturition. Nat Rev Neurosci. 2008;9(6):453–66.PubMedCentralCrossRefPubMed
Groen J, Pannek J, Castro-Diaz D, Del Popolo G, Gross T, Hamid R, et al. Summary of European Association of Urology (EAU) Guidelines on Neuro-Urology. Eur Urol. 2015 [Epub ahead of print].
Madhuvrata P, Singh M, Hasafa Z, Abdel-Fattah M. Anticholinergic drugs for adult neurogenic detrusor overactivity: a systematic review and meta-analysis. Eur Urol. 2012;62(5):816–30.CrossRefPubMed
Mangera A, Apostolidis A, Andersson KE, Dasgupta P, Giannantoni A, Roehrborn C, et al. An updated systematic review and statistical comparison of standardised mean outcomes for the use of botulinum toxin in the management of lower urinary tract disorders. Eur Urol. 2014;65(5):981–90.CrossRefPubMed
Panicker JN, Fowler CJ, Kessler TM. Lower urinary tract dysfunction in the neurological patient: clinical assessment and management. Lancet Neurol. 2015;14(7):720–32.